Uric Acid, Fructose and Hypertension
•
22 likes•8,660 views

Grand Rounds which summarizes the data pointing to fructose and sugar intake as the chief cause of hypertension and the use of allopurinal to treat pediatric hypertension.

Recommended
More Related Content
Viewers also liked
Similar to Uric Acid, Fructose and Hypertension
Similar to Uric Acid, Fructose and Hypertension (19)
More from Joel Topf
More from Joel Topf (20)
Recently uploaded
Recently uploaded (20)
Uric Acid, Fructose and Hypertension
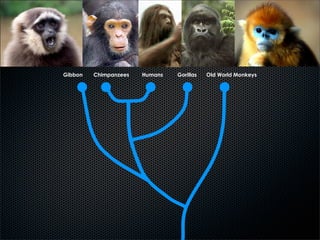
- 1. Gibbon Chimpanzees Humans Gorillas Old World Monkeys
- 2. nonsense mutation at codon 33 of urate oxidase Gibbon Chimpanzees Humans Gorillas Old World Monkeys 20 million years ago 25 million years ago
- 3. nonsense mutation at codon 33 of urate oxidase uric acid went from around 1 to 4 mg/dL Gibbon Chimpanzees Humans Gorillas Old World Monkeys 20 million years ago 25 million years ago
- 4. So humans, chimps and great apes separated themselves from all other mammals and joined reptiles and birds in being unable to convert uric acid to allantoin...
- 5. ...and twenty-five million years later this has resulted in the epidemic of hypertension
- 6. fructose, uric acid and hypertension Joel M. Topf, MD
- 10. 32% of americans are obese
- 11. 32% of americans are obese 110 years ago 3% were obese
- 14. lack of exercise? modeling calorie intake versus weight gain allows one to infer the effect of exercise In children all of the weight gain (1971-2002) was due to increase caloric consumption In adults the weight observed weight gain, 8.6 kg, was less than modeled from the increased caloric consumption due to increased activity Swinburn B. Increased energy intake alone virtually explains all the increase in body weight in the United States from the 1970s to the 2000s. 2009 European Congress on Obesity; May 6-9, 2009; Amsterdam, the Netherlands. Abstract T1:RS3.3.
- 15. lack of exercise? modeling calorie intake versus weight gain allows one to infer the effect of exercise In children all of the weight gain (1971-2002) was due to increase caloric consumption In adults the weight observed weight gain, 8.6 kg, was less than modeled from the increased caloric consumption due to increased activity Swinburn B. Increased energy intake alone virtually explains all the increase in body weight in the United States from the 1970s to the 2000s. 2009 European Congress on Obesity; May 6-9, 2009; Amsterdam, the Netherlands. Abstract T1:RS3.3.
- 17. The new normal: diabetes
- 19. 1898: William Osler reviewed 35,000 consecutive admissions to Johns Hopkins
- 20. 1898: William Osler reviewed 35,000 consecutive admissions to Johns Hopkins 10 had diabetes
- 21. 1898: William Osler reviewed 35,000 consecutive admissions to Johns Hopkins 10 had diabetes
- 22. 24 million americans have diabetes prevalence of diabetes has tripled from 1980 to 2006
- 23. 24 million americans have diabetes prevalence of diabetes has tripled from 1980 to 2006
- 24. hypertension Johnson et al. Potential role of sugar (fructose) in the epidemic of hypertension, obesity and the metabolic syndrome, diabetes, kidney disease, and cardiovascular disease. Am J Clin Nutr (2007) vol. 86 (4) pp. 899-906
- 25. 40% hypertension 30% 20% 10% 6% 0% 1907 1939 1975 1990 2004 Johnson et al. Potential role of sugar (fructose) in the epidemic of hypertension, obesity and the metabolic syndrome, diabetes, kidney disease, and cardiovascular disease. Am J Clin Nutr (2007) vol. 86 (4) pp. 899-906
- 26. 40% hypertension 30% 20% 10% 140/90 6% 0% 1907 1939 1975 1990 2004 Johnson et al. Potential role of sugar (fructose) in the epidemic of hypertension, obesity and the metabolic syndrome, diabetes, kidney disease, and cardiovascular disease. Am J Clin Nutr (2007) vol. 86 (4) pp. 899-906
- 27. 40% hypertension 30% 31% 28% 25% 20% 10% 12% 140/90 6% 0% 1907 1939 1975 1990 2004 Johnson et al. Potential role of sugar (fructose) in the epidemic of hypertension, obesity and the metabolic syndrome, diabetes, kidney disease, and cardiovascular disease. Am J Clin Nutr (2007) vol. 86 (4) pp. 899-906
- 28. diabetes + hypertension + obesity
- 30. 1940 Cardiology is established in the U.S. 1950 500 cardiologists in the United States 1960 World Health Organization pronounces a world epidemic of cardiovascular disease 2006 over 25,000 cardiologists in the United States 2006 1,000,000 coronary angiograms yearly 2006 720,000 cardiovascular surgeries yearly
- 31. Diabetes Hypertension Glomerulonephritis Polycystic disease Other 15%
- 32. 0% 100% 15% 1980 1981 1982 1983 1984 1985 Diabetes 1986 1987 1988 Polycystic disease 1989 1990 1991 Other 1992 1993 Hypertension 1994 1995 1996 1997 1998 1999 2000 2001 Glomerulonephritis 2002 2003 2004
- 33. 0% 100% 15% 1980 1981 1982 1983 1984 1985 Diabetes 1986 1987 1988 Polycystic disease 1989 1990 1991 Other 1992 1993 Hypertension 1994 1995 1996 1997 1998 1999 2000 2001 Glomerulonephritis 2002 2003 2004
- 34. 0% 100% 15% 1980 1981 1982 1983 1984 1985 Diabetes 1986 1987 1988 Polycystic disease 1989 1990 1991 Other 1992 1993 Hypertension 1994 1995 1996 1997 1998 1999 2000 2001 Glomerulonephritis 2002 2003 2004
- 35. 0% 100% 15% 1980 1981 1982 1983 1984 1985 Diabetes 1986 1987 1988 Polycystic disease 1989 1990 1991 Other 1992 1993 Hypertension 1994 1995 1996 1997 1998 1999 2000 2001 Glomerulonephritis 2002 2003 2004
- 36. 0% 100% 15% 1980 1981 1982 1983 1984 1985 Diabetes 1986 1987 1988 Polycystic disease 1989 1990 1991 Other 1992 1993 Hypertension 1994 1995 1996 1997 1998 1999 2000 2001 Glomerulonephritis 2002 2003 2004
- 37. 0% 100% 15% 1980 1981 1982 1983 1984 1985 Diabetes 1986 1987 1988 Polycystic disease 1989 1990 1991 Other 1992 1993 Hypertension 1994 1995 1996 1997 1998 1999 2000 2001 Glomerulonephritis 2002 2003 2004
- 38. Diabetes Hypertension Glomerulonephritis Polycystic disease Other
- 39. 0 10,000 20,000 30,000 40,000 50,000 1980 1981 1982 1983 1984 Diabetes 1985 1986 1987 Polycystic disease 1988 1989 1990 1991 Other 1992 1993 Hypertension 1994 1995 1996 1997 1998 1999 2000 2001 Glomerulonephritis 2002 2003 2004
- 40. 0 10,000 20,000 30,000 40,000 50,000 1980 1981 1982 1983 1984 Diabetes 1985 1986 1987 Polycystic disease 1988 1989 1990 1991 Other 1992 1993 Hypertension 1994 1995 1996 1997 1998 1999 2000 2001 Glomerulonephritis 2002 2003 2004
- 41. 0 10,000 20,000 30,000 40,000 50,000 1980 1981 1982 1983 1984 Diabetes 1985 1986 1987 Polycystic disease 1988 1989 1990 1991 Other 1992 1993 Hypertension 1994 1995 1996 1997 1998 1999 2000 2001 Glomerulonephritis 2002 2003 2004
- 42. 0 10,000 20,000 30,000 40,000 50,000 1980 1981 1982 1983 1984 Diabetes 1985 1986 1987 Polycystic disease 1988 1989 1990 1991 Other 1992 1993 Hypertension 1994 1995 1996 1997 1998 1999 2000 2001 Glomerulonephritis 2002 2003 2004
- 44. Sucrose glucose fructose relative sweetness sucrose lactose 16 galactose 32 glucose 50 high fructose corn honey 97 sucrose 100 syrup (HFCS) HFCS 42 100 fructose 173 0 50 100 150 200 on this scale saccharine would be 30,000 and aspartame 18,000
- 45. 10,000 years ago
- 46. Indians boil the cane juice and 500 B.C. produce crystal sugar
- 47. 1319 England sugar costs the equivalent of $100/kg medicinal 1493 Columbus brings sugar cane to the Caribbean Slave labor was imported from Africa to support the harvesting of sugar
- 48. 1319 England sugar costs the equivalent of $100/kg medicinal 1493 Columbus brings sugar cane to the Caribbean Slave labor was imported from Africa to support the harvesting of sugar
- 49. 1747: a German chemist, Andreas Marggraf discovered how to extract sugar crystals from sugarbeets During the British naval blockade during the Napoleonic wars sugarbeets became a major source of sugar
- 50. 1747: a German chemist, Andreas Marggraf discovered how to extract sugar crystals from sugarbeets During the British naval blockade during the Napoleonic wars sugarbeets became a major source of sugar world wide sugar production
- 51. 1866: Discovery of amylase Allows food precessors to convert corn starch into a syrup of pure glucose, corn syrup Since there is no fructose in corn syrup, it is not as sweet as sucrose
- 52. 1866: Discovery of amylase Allows food precessors to convert corn starch into a syrup of pure glucose, corn syrup Since there is no fructose in corn syrup, it is not as sweet as sucrose
- 54. 1960s: glucose (D-Xylose) isomerase is discovered. This enzyme converts glucose to fructose creating high fructose corn syrup
- 55. 1960s: glucose (D-Xylose) isomerase is discovered. This enzyme converts glucose to fructose creating high fructose corn syrup
- 56. 1960s: glucose (D-Xylose) isomerase is discovered. This enzyme converts glucose to fructose creating high fructose corn syrup
- 57. fructose compared to glucose increases triglycerides metabolized in the liver does not suppress appetite does not stimulate insulin release
- 58. fructose compared to glucose increases triglycerides metabolized in the liver does not suppress appetite does not stimulate insulin release HFCS compared with sucrose no difference in appetite cheaper no difference in insulin made in the USA no difference in triglycerides
- 60. 1700 Sugar Consumption 1 lb
- 61. 1700 Sugar Consumption 2000 Sugar Consumption 1 lb 70 lbs
- 63. sugar obesity diabetes sugar + hypertension and + obesity fructose
- 64. coincidencesugar or obesity diabetes sugar + causal? hypertension and + obesity fructose
- 65. diabetes + hypertension + obesity
- 66. diabetes + hypertension + obesity kidney disease heart disease
- 67. fructose diabetes + hypertension + obesity kidney disease heart disease
- 68. fructose fructose diabetes + uric acid hypertension + obesity kidney disease heart disease
- 69. fructose fructose diabetes + uric acid hypertension + obesity kidney disease heart disease
- 71. Glucose ATP hexokinase ADP Glucose-6-P Fructose 6-P ATP phosphofructokinase ADP Fructose 1,6 bisphosphate Dihydroxyacetone P Glyceraldehyde 3-P 1,3 Bisphosphoglycerate ADP ATP 3 Phosphoglycerate 2 Phosphoglycerate Phosphoenolpyruvate ADP pyruvate kinase ATP Pyruvate Hultman E, Nilsson LH, Sahlin K. Scand J Clin Lab Invest. 1975 May;35(3):245-51. Oberhaensli RD, Galloway GJ, Taylor DJ, Bore PJ, Radda GK. Br J Radiol. 1986 Jul;59(703):695-9.
- 72. Glucose ATP hexokinase ADP Glucose-6-P Fructose 6-P ATP phosphofructokinase ADP Fructose 1,6 bisphosphate Dihydroxyacetone P Glyceraldehyde 3-P 1,3 Bisphosphoglycerate ADP ATP 3 Phosphoglycerate 2 Phosphoglycerate Phosphoenolpyruvate ADP pyruvate kinase ATP Pyruvate Hultman E, Nilsson LH, Sahlin K. Scand J Clin Lab Invest. 1975 May;35(3):245-51. Oberhaensli RD, Galloway GJ, Taylor DJ, Bore PJ, Radda GK. Br J Radiol. 1986 Jul;59(703):695-9.
- 73. Glucose Fructose ATP hexokinase ATP ADP ADP Glucose-6-P Fructose-1-P Fructose 6-P Glyceraldehyde ATP + phosphofructokinase Dihydroxyacetone-P ADP Fructose 1,6 bisphosphate ATP ADP Dihydroxyacetone P Glyceraldehyde 3-P 1,3 Bisphosphoglycerate ADP ATP 3 Phosphoglycerate 2 Phosphoglycerate Phosphoenolpyruvate ADP pyruvate kinase ATP Pyruvate Hultman E, Nilsson LH, Sahlin K. Scand J Clin Lab Invest. 1975 May;35(3):245-51. Oberhaensli RD, Galloway GJ, Taylor DJ, Bore PJ, Radda GK. Br J Radiol. 1986 Jul;59(703):695-9.
- 74. Glucose Fructose In vitro: Fructose infusion for 70 ATP hexokinase ADP ATP ADP minutes resulted in 22.5% Glucose-6-P Fructose-1-P decrease in ATP, glucose did not change ATP Fructose 6-P Glyceraldehyde ATP + phosphofructokinase Dihydroxyacetone-P ADP Fructose 1,6 bisphosphate ATP ADP Dihydroxyacetone P Glyceraldehyde 3-P 1,3 Bisphosphoglycerate ADP ATP 3 Phosphoglycerate 2 Phosphoglycerate Phosphoenolpyruvate ADP pyruvate kinase ATP Pyruvate Hultman E, Nilsson LH, Sahlin K. Scand J Clin Lab Invest. 1975 May;35(3):245-51. Oberhaensli RD, Galloway GJ, Taylor DJ, Bore PJ, Radda GK. Br J Radiol. 1986 Jul;59(703):695-9.
- 75. Glucose Fructose In vitro: Fructose infusion for 70 ATP hexokinase ADP ATP ADP minutes resulted in 22.5% Glucose-6-P Fructose-1-P decrease in ATP, glucose did not change ATP Fructose 6-P Glyceraldehyde ATP + phosphofructokinase ADP Dihydroxyacetone-P In vivo: following a fructose load Fructose 1,6 bisphosphate ATP ADP hepatic fructose-1-P rose 800% and ATP fell 75% Dihydroxyacetone P Glyceraldehyde 3-P 1,3 Bisphosphoglycerate ADP ATP 3 Phosphoglycerate 2 Phosphoglycerate Phosphoenolpyruvate ADP pyruvate kinase ATP Pyruvate Hultman E, Nilsson LH, Sahlin K. Scand J Clin Lab Invest. 1975 May;35(3):245-51. Oberhaensli RD, Galloway GJ, Taylor DJ, Bore PJ, Radda GK. Br J Radiol. 1986 Jul;59(703):695-9.
- 76. Every fructose molecule available is consumed in an unregulated metabolic fire burning all available ATP in the process Consumption can consume all of the ATP leading to Lactic acidosis Ischemia Lots and lots of adenosine, a purine
- 77. Glucose Fructose In vitro: Fructose infusion for 70 ATP hexokinase ADP ATP ADP minutes resulted in 22.5% Glucose-6-P Fructose-1-P decrease in ATP, glucose did not change ATP Fructose 6-P Glyceraldehyde ATP + phosphofructokinase ADP Dihydroxyacetone-P In vivo: following a fructose load Fructose 1,6 bisphosphate ATP ADP hepatic fructose-1-P rose 800% and ATP 75% Dihydroxyacetone P Glyceraldehyde 3-P 21 men placed on a diet 1,3 Bisphosphoglycerate containing 25-30% of calories ADP ATP from sucrose developed 3 Phosphoglycerate increase in SGPT, SGOT within 18 days. Transaminases 2 Phosphoglycerate normalized with 10% of calories Phosphoenolpyruvate from sucrose ADP pyruvate kinase ATP Hultman E, Nilsson LH, Sahlin K. Scand J Clin Lab Invest. 1975 Pyruvate May;35(3):245-51. Oberhaensli RD, Galloway GJ, Taylor DJ, Bore PJ, Radda GK. Br J Radiol. 1986 Jul;59(703):695-9. Porikos KP, Van Itallie TB. Am J Med. 1983 Oct;75(4):624-30.
- 78. Fructose and non-alcoholic fatty liver disease 16-23% of Americans have non- alcoholic fatty liver disease Ouyang X, Cirillo P, Sautin Y, McCall S, Bruchette JL, Diehl AM, Johnson RJ, Abdelmalek MF. J Hepatol. 2008 June; 48(6): 993–999.
- 79. Fructose and non-alcoholic fatty liver disease 16-23% of Americans have non- alcoholic fatty liver disease Daily fructose intake (cal/day) Ouyang X, Cirillo P, Sautin Y, McCall S, Bruchette JL, Diehl AM, Johnson RJ, Abdelmalek MF. J Hepatol. 2008 June; 48(6): 993–999.
- 80. Fructose and non-alcoholic fatty liver disease 16-23% of Americans have non- alcoholic fatty liver disease Daily fructose intake (cal/day) NHANES 1999-2000 Ouyang X, Cirillo P, Sautin Y, McCall S, Bruchette JL, Diehl AM, Johnson RJ, Abdelmalek MF. J Hepatol. 2008 June; 48(6): 993–999.
- 81. Fructose and non-alcoholic fatty liver disease 16-23% of Americans have non- alcoholic fatty liver disease Daily fructose intake (cal/day) NHANES 1999-2000 Uric Acid was 41% higher in patients with NAFLD (p<0.03) Ouyang X, Cirillo P, Sautin Y, McCall S, Bruchette JL, Diehl AM, Johnson RJ, Abdelmalek MF. J Hepatol. 2008 June; 48(6): 993–999.
- 82. Fructose and non-alcoholic fatty liver disease 16-23% of Americans have non- alcoholic fatty liver disease Daily fructose intake (cal/day) NHANES 1999-2000 Uric Acid was 41% higher in patients with NAFLD (p<0.03) Ouyang X, Cirillo P, Sautin Y, McCall S, Bruchette JL, Diehl AM, Johnson RJ, Abdelmalek MF. J Hepatol. 2008 June; 48(6): 993–999.
- 83. Ouyang X, Cirillo P, Sautin Y, McCall S, Bruchette JL, Diehl AM, Johnson RJ, Abdelmalek MF. J Hepatol. 2008 June; 48(6): 993–999.
- 84. glycolysis Intermediates AMP GMP Consumption of ATP PRPP Adenosine Guanosine creates adenosine, a purine IMP Inosine Guanine All purines are Hypoxanthine Xanthine oxidase metabolized to uric acid by xanthine Xanthine oxidase Xanthine oxidase Uric Acid
- 85. glycolysis Intermediates AMP GMP Consumption of ATP PRPP Adenosine Guanosine creates adenosine, a purine IMP Inosine Guanine All purines are Hypoxanthine Xanthine oxidase metabolized to uric acid by xanthine Xanthine oxidase Xanthine oxidase Uric Acid
- 86. Stirpe et al. Fructose-induced hyperuricaemia. Lancet (1970) vol. 2 (7686) pp. 1310-1
- 87. 6 5.9 5.7 5.6 Uric Acid (mg/dL) 5 fructose (g/kg) equal to a liter of pepsi for a 70 kg 4.4 woman 4 0 30 60 120 Time (minutes) Stirpe et al. Fructose-induced hyperuricaemia. Lancet (1970) vol. 2 (7686) pp. 1310-1
- 88. Perheentupa and Raivio. Fructose-induced hyperuricaemia. Lancet (1967) vol. 2 (7515) pp. 528-31
- 89. fructose (0.5 g/kg) IV infusion peak uric acid was seen within 15 minutes and persisted over 5 hours Perheentupa and Raivio. Fructose-induced hyperuricaemia. Lancet (1967) vol. 2 (7515) pp. 528-31
- 90. If fructose increases uric acid, and fructose consumption has sky rocketed in the last few decades, are we seeing more gout?
- 91. 10.0 7.5 gout/1000 patients gout in England 5.0 2.5 0 1970/71 1981/82 1991 Harris et al. The prevalence and prophylaxis of gout in England. J Clin Epidemiol (1995) vol. 48 (9) pp. 1153-8
- 92. Arromdee et al. Epidemiology of gout: is the incidence rising?. J Rheumatol (2002) vol. 29 (11) pp. 2403-6
- 93. Arromdee et al. Epidemiology of gout: is the incidence rising?. J Rheumatol (2002) vol. 29 (11) pp. 2403-6
- 94. 1977 VERSUS 1995 Arromdee et al. Epidemiology of gout: is the incidence rising?. J Rheumatol (2002) vol. 29 (11) pp. 2403-6
- 95. Annual Incidence 70.0 1977-78 1995-96 p 62 52.5 age 43.5 53.5 0.07 New cases/100,000 45 weight 84.5 85.5 0.50 42 35.0 BMI 28.8 29.8 0.36 17.5 uric acid 8.3 8.4 0.28 16 0 all cases no HCTZ 1977-78 1995-96
- 98. 1.Fructose increases uric acid 2.Uric acid and gout are increasing increasing 3.Uric acid causes hypertension circumstantial animal interventional
- 101. Uric acid causes hypertension Uric acid is associated but doesn’t cause hypertension
- 105. prospective trial total and CV mortality based on baseline uric acid 6,763 participants in the Framingham Heart Study no association in men positive association in women when adjusted for: age, BMI, SBP, use of antihypertensive agents, use of diuretics, diabetes, cholesterol level, smoking status, alcohol intake, LVH, and menopausal status the data in women was no longer significant Culleton et al. Serum uric acid and risk for cardiovascular disease and death: the Framingham Heart Study. Ann Intern Med (1999) vol. 131 (1) pp. 7-13
- 106. NHANES I n=5,926 after excluding prior CVD, gout, or currently pregnant 16.4 years follow-up 1,293 deaths 731 CVD 429 Cancer Fang and Alderman. Serum uric acid and cardiovascular mortality the NHANES I epidemiologic follow-up study, 1971-1992. National Health and Nutrition Examination Survey. JAMA (2000) vol. 283 (18) pp. 2404-10
- 107. NHANES I n=5,926 after excluding prior CVD, gout, or currently pregnant 16.4 years follow-up 1,293 deaths 731 CVD 429 Cancer Fang and Alderman. Serum uric acid and cardiovascular mortality the NHANES I epidemiologic follow-up study, 1971-1992. National Health and Nutrition Examination Survey. JAMA (2000) vol. 283 (18) pp. 2404-10
- 108. Fang and Alderman. Serum uric acid and cardiovascular mortality the NHANES I epidemiologic follow-up study, 1971-1992. National Health and Nutrition Examination Survey. JAMA (2000) vol. 283 (18) pp. 2404-10
- 109. Fang and Alderman. Serum uric acid and cardiovascular mortality the NHANES I epidemiologic follow-up study, 1971-1992. National Health and Nutrition Examination Survey. JAMA (2000) vol. 283 (18) pp. 2404-10
- 110. For each increase in the uric acid of one Fang and Alderman. JAMA (2000) vol. 283 (18) pp. 2404-10
- 111. MEN Death from CVD rose 9% Fatal MI increased 17% For each increase in the uric acid of one WOMEN Death from CVD rose 26% Fatal MI increased 30% Fang and Alderman. JAMA (2000) vol. 283 (18) pp. 2404-10
- 112. Uric acid causes hypertension Uric acid is associated but doesn’t cause hypertension
- 113. increased uric acid Uric acid causes hypertension kidney disease Uric acid is associated but doesn’t cause hypertension hypertension
- 114. increased uric acid hypertension Uric acid causes hypertension kidney disease kidney disease Uric acid is associated but doesn’t cause hypertension hypertension increased uric acid
- 115. Framingham population 3,329 subjects had blood pressure and uric acid assessed 4 years later the blood pressure was reassessed analysis looked at the patients who developed new hypertension or had their hypertension become more severe Sundström et al. Relations of serum uric acid to longitudinal blood pressure tracking and hypertension incidence. Hypertension (2005) vol. 45 (1) pp. 28-33
- 116. An increase in the uric acid of 1.2 mg/dL increased risk of worsening hypertension by 27% Developed Hypertension Worsening Hypertension 20 40 15 35 10 30 5 25 0 20 1st 2nd 3rd 4th 1st 2nd 3rd 4th Sundström et al. Relations of serum uric acid to longitudinal blood pressure tracking and hypertension incidence. Hypertension (2005) vol. 45 (1) pp. 28-33
- 117. 1.Fructose increases uric acid 2.Uric acid and gout are increasing increasing 3.Uric acid causes hypertension circumstantial animal interventional
- 118. The problem with animal models: uricase or urate oxidase Uric acid + O2 + H2O → 5-hydroxyisourate + H2O2→ allantoin + CO2 Normal rat uric acid is 1 mg/dL
- 119. The problem with animal models: uricase or urate oxidase Uric acid + O2 + H2O → 5-hydroxyisourate + H2O2→ allantoin + CO2 Normal rat uric acid is 1 mg/dL You need to feed them oxanic acid, which inhibits uricase. ๏ Give too much, the rat dies of urate nephropathy ๏ Give too little and the uric acid remains too low ๏ Titrate dose and you can safely double the uric acid
- 120. normal salt diet Mice randomized to Control Oxanic acid control diet or oxanic 151 acid Oxanic acid doubles p=0.05 Systolic BP p=0.05 the serum uric acid 130 Within a month, a significant increase in blood pressure 109 Baseline 4 weeks 7 weeks Mazzali et al. Hypertension (2001) vol. 38 (5) pp. 1101-6
- 121. All mice are fed a low Control Oxanic acid salt diet Oxanic Acid + Allopurinol Then randomized to diet alone, oxanic acid or oxanic acid plus allopuriniol If the culprit is uric acid, allopurinol should neutralize it Mazzali et al. Hypertension (2001) vol. 38 (5) pp. 1101-6
- 122. All mice are fed a low Control Oxanic acid salt diet Oxanic Acid + Allopurinol 151 Then randomized to diet alone, oxanic acid or Systolic BP oxanic acid plus 130 allopuriniol If the culprit is uric acid, allopurinol should 109 neutralize it Baseline week 2 week 4 week 5 week 7 Mazzali et al. Hypertension (2001) vol. 38 (5) pp. 1101-6
- 123. All mice are fed a low Control Oxanic acid salt diet Oxanic Acid + Allopurinol 151 Then randomized to diet alone, oxanic acid or Systolic BP oxanic acid plus 130 allopuriniol If the culprit is uric acid, allopurinol should 109 neutralize it Baseline week 2 week 4 week 5 week 7 Mazzali et al. Hypertension (2001) vol. 38 (5) pp. 1101-6
- 124. All mice are fed a low Control Oxanic acid salt diet Oxanic Acid + Allopurinol 151 Then randomized to diet alone, oxanic acid or Systolic BP oxanic acid plus 130 allopuriniol If the culprit is uric acid, allopurinol should 109 neutralize it Baseline week 2 week 4 week 5 week 7 Mazzali et al. Hypertension (2001) vol. 38 (5) pp. 1101-6
- 125. Control Oxanic acid Oxanic Acid + Allopurinol 151 Systolic BP 130 109 Baseline week 2 week 4 week 5 week 7 Mazzali et al. Hypertension (2001) vol. 38 (5) pp. 1101-6
- 126. Control Oxanic acid Mice randomized to Oxanic Acid + Benziodarone control, oxanic acid or oxanic acid + benziodarone benziodarone is a uricosuric agent so it can decrease uric acid without affecting xanthine oxidase Mazzali et al. Hypertension (2001) vol. 38 (5) pp. 1101-6
- 127. Control Oxanic acid Mice randomized to Oxanic Acid + Benziodarone control, oxanic acid or 170 oxanic acid + benziodarone Systolic BP 135 benziodarone is a uricosuric agent so it can decrease uric acid without affecting 100 Baseline week 2 week 3 week 4 week 5 week 6 week7 xanthine oxidase Mazzali et al. Hypertension (2001) vol. 38 (5) pp. 1101-6
- 128. Control Oxanic acid Mice randomized to Oxanic Acid + Benziodarone control, oxanic acid or 170 oxanic acid + benziodarone Systolic BP 135 benziodarone is a uricosuric agent so it can decrease uric acid without affecting 100 Baseline week 2 week 3 week 4 week 5 week 6 week7 xanthine oxidase Mazzali et al. Hypertension (2001) vol. 38 (5) pp. 1101-6
- 129. Control Oxanic acid Oxanic Acid + Benziodarone 170 Systolic BP 135 10 mg/kg 15 mg/kg 100 Baseline week 2 week 3 week 4 week 5 week 6 week7 Mazzali et al. Hypertension (2001) vol. 38 (5) pp. 1101-6
- 130. Correction of hyperuricemia after 7 weeks Oxanic Acid Oxanic Acid -> Withdrawl Oxanic Acid ->Allopurinol Mazzali et al. Hypertension (2001) vol. 38 (5) pp. 1101-6
- 131. Correction of hyperuricemia after 7 weeks Oxanic Acid Oxanic Acid -> Withdrawl Oxanic Acid ->Allopurinol 170 Systolic BP 135 100 Baseline week 2 week 4 week 6 week 7 week 8 week 9 week 10 week 11 Mazzali et al. Hypertension (2001) vol. 38 (5) pp. 1101-6
- 132. Correction of hyperuricemia after 7 weeks Oxanic Acid Oxanic Acid -> Withdrawl Oxanic Acid ->Allopurinol 170 Systolic BP 135 100 Baseline week 2 week 4 week 6 week 7 week 8 week 9 week 10 week 11 Mazzali et al. Hypertension (2001) vol. 38 (5) pp. 1101-6
- 133. Correction of hyperuricemia after 7 weeks Oxanic Acid Oxanic Acid -> Withdrawl Oxanic Acid ->Allopurinol 170 Systolic BP 135 100 Baseline week 2 week 4 week 6 week 7 week 8 week 9 week 10 week 11 Mazzali et al. Hypertension (2001) vol. 38 (5) pp. 1101-6
- 134. uric acid can account 56% of the variability in blood pressure Mazzali et al. Hypertension (2001) vol. 38 (5) pp. 1101-6
- 135. At 7 weeks, the renal function and routine light microscopy was unremarkable... However, immunohistochemical stains revealed early interstitial fibrosis and tubular injury. The administration of allopurinol... prevented... significant these low-grade but inflammatory and fibrotic changes. Mazzali et al. Hypertension (2001) vol. 38 (5) pp. 1101-6
- 136. 0 40 80 120 160 Control Renin % +JGA Oxanic Acid NOS1 cells/100 Glom Oxanic Acid + Allopurinol 0 30 60 90 120 Control Oxanic Acid Renin % +JGA Oxalanic acid withdrawal NOS1 cells/100 Glom Oxanic Acid + Allopurinol
- 137. Renin % +JGA Renin % +JGA NOS1 cells/100 Glom NOS1 cells/100 Glom 160 120 120 hypertension driven by 90 Renin 80 60 40 30 NO 0 0 Control Oxanic Acid Oxanic Acid + Allopurinol Control Oxanic Acid Oxalanic acid withdrawal Oxanic Acid + Allopurinol
- 138. 1.Fructose increases uric acid 2.Uric acid and gout are increasing increasing 3.Uric acid causes hypertension circumstantial animal interventional
- 139. Human interventional data Ideal test subjects Homogenous population No comorbidities to complicate interpretation New onset disease without end-organ damage
- 142. What disease is the type I diabetes of hypertension?
- 143. What disease is the type I diabetes of hypertension?
- 144. What disease is the type I diabetes of hypertension? Pediatric primary hypertension
- 145. Secondary hypertension Primary Secondary renal disease cardiac disease endocrine disease represents 30-60% of pediatric hypertension
- 146. 125 consecutive referrals to the pediatric renal division for hypertension were enrolled in trial After a hypertension work-up the diagnosis were: Primary hypertension: 63 Secondary hypertension: 40 White coat hypertension: 22 Primary Secondary White Coat Hypertension Feig and Johnson. Hypertension (2003) vol. 42 (3) pp. 247-52
- 147. uric acid levels by diagnosis 6.7 4.3 3.5 3.6 Feig and Johnson. Hypertension (2003) vol. 42 (3) pp. 247-52
- 148. uric acid levels by diagnosis 6.7 3.5 3.6 Feig and Johnson. Hypertension (2003) vol. 42 (3) pp. 247-52
- 149. uric acid levels by diagnosis essential normal (control or hypertension white coat) 100% 56 uric acid > 5.5 56 0 ppv 56+0 89% 62 uric acid ≤ 5.5 7 62 npv 62+7 88% sensitive 100% specific 56 62 56+7 62+0 6.7 3.5 3.6 Feig and Johnson. Hypertension (2003) vol. 42 (3) pp. 247-52
- 150. uric acid levels by diagnosis 6.7 4.3 3.5 3.6 Feig and Johnson. Hypertension (2003) vol. 42 (3) pp. 247-52
- 151. uric acid levels by diagnosis pathology normal (control or (1° or 2°) white coat) 100% 68 uric acid > 5.5 68 0 ppv 68+0 63% 62 uric acid ≤ 5.5 36 62 npv 62+36 65% sensitive 100% specific 68 62 68+36 62+0 6.7 4.3 3.5 3.6 Feig and Johnson. Hypertension (2003) vol. 42 (3) pp. 247-52
- 152. uric acid levels by diagnosis 6.7 4.3 Feig and Johnson. Hypertension (2003) vol. 42 (3) pp. 247-52
- 153. uric acid levels by diagnosis essential secondary hypertension hypertension 82% 56 uric acid > 5.5 56 12 ppv 56+12 80% 28 uric acid ≤ 5.5 7 28 npv 28+7 88% sensitive 70% specific 56 28 56+7 28+12 6.7 4.3 Feig and Johnson. Hypertension (2003) vol. 42 (3) pp. 247-52
- 154. uric acid levels by diagnosis essential secondary hypertension hypertension 82% 56 uric acid > 5.5 56 12 ppv 56+12 80% 28 uric acid ≤ 5.5 7 28 npv 28+7 88% sensitive 70% specific 56 28 56+7 28+12 6.7 4.3 renal ultrasound with Doppler DMSA renal perfusion scan renin and aldosterone levels renal angiogram Urinary catecholamines Feig and Johnson. Hypertension (2003) vol. 42 (3) pp. 247-52
- 155. allopurinol to treat hypertension if uric acid causes hypertension then reducing uric acid should treat hypertension that’s impossible allopurinol can’t treat hypertension
- 157. Randomized, double- blind, placebo-controlled, crossover trial of allopurinol in children with newly diagnosed essential hypertension Aged 11 - 17 BP in the 95th percentile for sex, age, and height excluded stage II hypertension (SBP > 99% + 5) Serum uric acid level of 6 mg/dL or higher No evidence for target organ damage or secondary hypertension No current or prior treatment with an hypertensive medication for any indication
- 158. Allopurinol 200 mg bid placebo 4 weeks 4 weeks
- 159. 73% over weight or obese 30% met criteria for metabolic syndrome
- 160. 73% over weight or obese 30% met criteria for metabolic syndrome
- 161. 0 3 6 9 enrollment begin placebo end placebo uric acid begin allopurinol end allopurinol
- 162. 115 125 135 145 enrollment begin placebo in-clinic end placebo systolics begin allopurinol 24-hr end allopurinol 60 70 80 90 enrollment begin placebo in clinic end placebo diastolics begin allopurinol 24-hr end allopurinol
- 163. 20 of the 30 participants achieved normal BP during the allopurinol phase, whereas only 1 of 30 achieved normal BP during the placebo phase. Of the 10 participants who remained hypertensive while taking allopurinol, 7 had a uric acid level of 5.0 mg/dL or higher at the end of the allopurinol phase.
- 164. The new normal
- 165. if uric acid is so bad for us, why are we among the only mammals without uricase?
- 166. Gibbon Chimpanzees Humans Gorillas Orangutans Old World Monkeys Urate oxidase genes nonsense: codon 33 nonsense: codon 187 aberrant splice 13-bp deletion
- 167. Gibbon Chimpanzees Humans Gorillas Orangutans Old World Monkeys Urate oxidase genes nonsense: codon 33 nonsense: codon 187 aberrant splice 13-bp deletion
- 168. Gibbon Chimpanzees Humans Gorillas Orangutans Old World Monkeys Urate oxidase genes nonsense: codon 33 nonsense: codon 187 aberrant splice 13-bp deletion
- 169. Gibbon Chimpanzees Humans Gorillas Orangutans Old World Monkeys Urate oxidase genes nonsense: codon 33 nonsense: codon 187 aberrant splice 13-bp deletion
- 170. Gibbon Chimpanzees Humans Gorillas Orangutans Old World Monkeys Urate oxidase genes nonsense: codon 33 nonsense: codon 187 aberrant splice 13-bp deletion
- 171. Gibbon Chimpanzees Humans Gorillas Orangutans Old World Monkeys Urate oxidase genes nonsense: codon 33 nonsense: codon 187 aberrant splice 13-bp deletion
- 172. Gibbon Chimpanzees Humans Gorillas Orangutans Old World Monkeys Urate oxidase genes nonsense: codon 33 nonsense: codon 187 aberrant splice 13-bp deletion
- 173. Because the disruption of a functional gene by independent events in two different evolutionary lineages is unlikely to occur on a chance basis, our data favor the hypothesis that the loss of urate oxidase may have evolutionary advantages. Wu XW, Muzny DM, Lee CC, Caskey CT. Mol Evol. 1992 Jan;34(1):78-84.
- 174. twice evolution selected for a loss of uricase perhaps our Paleolithic diet was so low in sodium and potassium rich that having a higher blood pressure thanks to uric acid was advantageous perhaps we are currently living in the new normal where uric acid, after long being selected for, is now harmful
- 175. addendum what should we do about asymptomatic hyperuricemia?
- 176. allopurinol for hyperuricemia retrospective analysis of allopurinol use in patients with uric acid >7 mg/dL 9,924 veterans 2,483 subjects received allopurinol 7,441 in the control group Luk et al. Allopurinol and mortality in hyperuricaemic patients. Rheumatology (2009) vol. 48 (7) pp. 804-806
- 178. allopurinol 23% lower mortality
- 179. thanks pbfluids.com
Editor's Notes
- glucose can be metabolized by every tissue fructose a 5 carbon carbohydrate. metabolized primarily by the liver sucrose (table sugar) is a disaccharide of fructose and glucose HFCS is a mixture of 45-52% fructose with the balance being glucose
- fresh biopsies bathed in various concentrations of fructose MR spectroscopy
- fresh biopsies bathed in various concentrations of fructose MR spectroscopy
- fresh biopsies bathed in various concentrations of fructose MR spectroscopy
- fresh biopsies bathed in various concentrations of fructose MR spectroscopy
- fresh biopsies bathed in various concentrations of fructose MR spectroscopy
- fresh biopsies bathed in various concentrations of fructose MR spectroscopy
- fresh biopsies bathed in various concentrations of fructose MR spectroscopy
- rasbiuricase or elitek $2,724.84
- benzee oda rone a uricosuric agent like probenacid
- benzee oda rone a uricosuric agent like probenacid
- benzee oda rone a uricosuric agent like probenacid
- benzee oda rone a uricosuric agent like probenacid
- benzee oda rone a uricosuric agent like probenacid
- benzee oda rone a uricosuric agent like probenacid