Coronary Ostial stenting techniques:Current status
•Download as PPTX, PDF•
51 likes•16,007 views

Ostial lesions, located within 3 mm of a vessel origin, pose unique challenges for percutaneous coronary intervention (PCI). Precise stent placement is required to avoid geographic miss and ensure optimal coverage of the lesion. Several techniques have been developed to aid accurate stent placement for ostial lesions, including aorto-free floating wire, stent pull-back, and Szabo/anchor wire methods. The use of these targeted approaches can reduce the risk of additional stenting and reintervention compared to conventional PCI for ostial lesions.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Coronary Ostial stenting techniques:Current status
Similar to Coronary Ostial stenting techniques:Current status (20)
Recently uploaded
Recently uploaded (20)
Coronary Ostial stenting techniques:Current status
- 1. Ostial stenting techniques Dr Pawan Kumar Ola PGIMER,Dr RML Hospital New Delhi
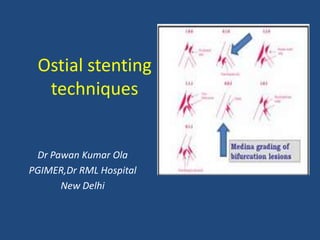
- 2. • Ostial lesion- within 3 mm of the vessel origin. • Classification based on location:- Aorto-ostial Non aorto-ostial Branch ostial
- 4. • Isolated aorto-ostial disease is more frequent in women and is more common at the RCA than at the LMS. Stewart JT, Eur Heart J. 1987;8:917-20 Rissanen V, Br Heart J. 1975;37:182-91 • Causes- Atherosclerotic (accompanying downstream plaque) Aortitis (syphilis or Takayasu arteritis) Mediastinal radiotherapy
- 5. • Ostial lesions are usually fibrotic, calcified, and relatively rigid. • Aorto-ostial disease is felt to be additionally resistant to dilatation and prone to recoil due to the greater thickness of muscular and elastic tissue in the aortic wall. Popma JJ, Am J Cardiol 1991;67:431-3
- 6. • Ostial lesions including Aorto-ostial and Medina 001, are difficult to treat. • PCI of an ostial lesion requires precise implantation of a stent in order to prevent adverse clinical outcomes. • “Geographic miss” occurs when the ostial side- branch lesion is not fully covered by the stent.
- 7. • Conversely, a stent placed too proximal into the main vessel may complicate future coronary intervention or lead to acute problems in the main branch. Comparison of outcomes of percutaneous coronary intervention of ostial versus nonostial narrowing of the major epicardial coronary arteries Am J Cardiol. 2004;94:583-587
- 8. We evaluated data from all PCIs performed from 1998 to 2001 in the proximal segments of the major epicardial coronary arteries entered into a large cardiac database and compared ostial with nonostial PCI outcomes. Of 2,484 patients who underwent PCI of a proximal coronary artery (left anterior descending, left circumflex, or right coronary), 223 patients had ostial narrowing and 2,261 patients had proximal, nonostial narrowing. Baseline characteristics were similar between the 2 groups. Stenting occurred in 89% of all patients and was similar in patients with ostial or nonostial narrowings. Procedural success was the same for ostial and nonostial PCI (96% vs 95%, p = 0.95). One-year event-free survival rate was lower in patients who underwent ostial PCI (69% vs 80%, p = 0.0019), largely due to a greater need for repeat PCI (19% vs 10%, p <0.0001). Multivariate analysis showed that ostial location, age, angina class, and number of diseased vessels were independent predictors of the occurrence of cardiac events. Am J Cardiol. 2004;94:583-587
- 9. Additional judgements…… • Exclusion of coronary spasm- • Ostial LAD stenosis- Whether precise positioning of the stent at the ostium should be attempted or stenting across the Cx back into the LMS ?
- 10. Technical considerations for ostial LAD stenosis Presence or absence of an ostial ‘nub’ or stump… Angle of bifurcation- angles <75 ̊ associated with greater difficulty in stent positioning and increased risk of plaque shift.
- 11. Presence of significant plaque in the distal LM or CX ostium… Presence of heavy calcification…
- 12. • Side-branch ostial stenosis- The balance of risk vs. benefit may favour medical therapy. Am J Cardiol 2004;93:1162–1164
- 13. • Total 302 patients of isolated stenosis of diagonal branches ≥2 mm included (Medical 233 vs. 69 angioplasty). Am J Cardiol 2004;93:1162–1164
- 14. Conclusion: PCI of ostial stenosis of diagonal branches in patients without further significant coronary artery stenoses did not reduce adverse cardiac events, nor did it result in a greater portion of freedom from angina pectoris
- 15. • Ostial stenosis following previous bifurcation PCI… - to establish whether the ostium was originally covered and whether stent sizing and expansion was optimal.
- 17. Intravascular Ultrasound Ability to confirm or refute the presence of significant aorto-ostial disease. Assessment of vessel size to guide stent selection Assessment of adequacy of stent expansion Assessment of degree of calcification and need for adjunctive devices Assessment of ostial site restenosis To assess for the presence of proximal or branch vessel disease prior to deciding on a treatment strategy
- 18. • IVUS is non-physiological • Guidecatheter disengagement during pullback risks non-coaxial imaging of the ostium and overestimation of the luminal area.
- 19. JACC Interv. 2013; Vol.6 (2) Suppl
- 21. “Eyebrow Sign” Medina A et al.Rev Esp Cardiol. 2009;62(11):1240-9 peculiar spiky morphology termed the “eyebrow sign”.
- 22. baseline and post-treatment ultrasound studies showing the “eyebrow sign” (arrow) and carina displacement (arrow heads). IVUS examination showing the carina without the “eyebrow sign” Medina A et al.Rev Esp Cardiol. 2009;62(11):1240-9
- 23. Fractional flow reserve (FFR) FFR in aorto-ostial disease may be valuable, but it requires: (a) initial pressure equalisation in the ascending aorta prior to vessel engagement (b) guide catheter disengagement during FFR measurement so as not to occlude flow; (c) ideally, an intravenous infusion of adenosine rather than an intracoronary bolus, as the latter requires catheter engagement to allow selective injection and flush followed by rapid disengagement to allow FFR measurement.
- 24. • Hyperemia induced with an intracoronary bolus administration (80 ug in left coronary artery, 40ug in right coronary artery) or intravenous infusion (140ug/kg/min) of adenosine. • Branch-ostial disease – Studies measuring fractional flow reserve (FFR) have frequently shown a lack of relation between apparent angiographic severity of side-branch ostial disease and ability to cause ischaemia. Ziaee A et al. Am J Cardiol 2004;93:1404-7, A9. Lim MJ et al. Catheter Cardiovasc Interv 2005;65:461-8
- 26. Before Ostial side branch PCI we should know….. What is the size of the side branch and the area of myocardium supplied? What is the significance of the degree of stenosis of the ostial lesion and is there evidence of ischemia either based on stress testing or clinical symptoms that warrant treatment? Would fractional flow reserve be required since the side- branch procedure may jeopardize the main branch?
- 27. Guide catheter • For aorto-ostial lesions less aggressive catheters like Judkins, are recommended to avoid deep engagement and to facilitate disengagement during stent placement.
- 28. • For aorto-coronary bypass grafts, a guide catheter which provides adequate reach and support without deep intubation is required. • Judkins right, Multipurpose, RCB, LCB and Amplatz left catheters are commonly used.
- 29. Additional distal disease should be treated first. Side-hole catheters, although commonly used, are not recommended as the warning sign of pressure damping from catheter wedging and occlusion of flow is obscured. For intervention on aorto‐ostial disease, it is advisable to preload the wire in the guide before vessel Intubation - to facilitate rapid wiring and catheter disengagement if necessary.
- 30. Lesion Preparation & Debulking • Greater calcification and lesion rigidity at ostial sites plus the risk of significant plaque shift may dictate a plaque modification or debulking strategy. • Cutting balloon (Flextome),Scoring balloon (AngioSculpt) and Rotational Atherectomy may be considered.
- 31. Angiographic Views Vessel with ostial lesion Suggested view LMS AP cranial or LAO cranial RCA LAO or ideally LAO caudal to demonstrate the plane of the ostium LAD A combination of caudal views (LAO caudal typically shows least overlap with ramus or Cx but is more foreshortened than the RAO caudal view). Cx LAO caudal usually best, but if overlap present, LAO cranial may help Bypass graft Usually LAO ± caudal for RCA grafts (as for native RCA) For LCA grafts, the ostium is usually least foreshortened in an RAO view
- 32. Ostial lesions PCI techniques
- 33. Angiographically assisted Stent placement • Most common technique used • Precise stent placement is very difficult • Large volume of contrast & multiple views required
- 34. • In a retrospective analysis of 100 ostial lesions, Dishmon et al found that the true ostium was missed in 54% of cases. • Proximal miss was found in 52%, resulting in the inability to engage the guiding catheter in 93% of cases. • Distal miss was found in 48% of cases, resulting in additional stents for 38% of cases. • Furthermore, the target lesion revascularization (TLR) rates were increased 3-fold when compared to patients without geographic miss. Dishmon DA et al.J Invasive Cardiol. 2011;23(8):322-326.
- 35. Aorta free-floating wire technique (for aorta-ostial lesion only) “Sepal Wire Technique” — A Novel Technique for Aorto-ostial Left Main Stenting Chan et al. J INVASIVE CARDIOL 2011;23:211–212
- 36. The guide catheter is backed out of the ostium and the second wire is advanced into the aorta. This second wire acts as a marker for the ostium and prevents the guide from deeply engaging the vessel
- 37. JACC Interv. 2014;Vol 7 (25) Suppl.
- 38. Stent draw-back technique Schwartz L, Morsi A. J Invasive Cardiol 2002;14:66-71. (a) The stent is advanced on the target vessel wire beyond the lesion; (b) a balloon is advanced over the second wire opposite the ostium of the target vessel; (c) the balloon is then inflated at low pressure (6-8 atm); (d) the undeployed stent catheter is pulled back against the inflated balloon until a dent is seen; (e) both balloons are deflated.
- 39. Schwartz L, Morsi A. J Invasive Cardiol 2002;14:66-71.
- 40. American Journal of Cardiology Volume 96, Issue 8 , Pages 1123-1128, 15 October 2005 Effectiveness of the Stent Pull-Back Technique for Nonaorto Ostial Coronary Narrowings •Annapoorna S. Kini, Pedro R. Moreno, Angelica M. Steinheimer Samin K. Sharma, MD Cardiac Catheterization Laboratory of the Cardiovascular Institute, Mount Sinai Hospital, New York, New York Coronary stenting of nonaorto ostial coronary lesions is challenging because of plaque shift into the main vessel, triggering the use of additional stents. Furthermore, inappropriate coverage of the ostium of the side branch increases the risk of restenosis and target vessel revascularization (TVR). To improve the treatment of nonaorto ostial coronary lesions with a novel interventional technique, we tested the hypothesis that inflating a balloon in the main vessel before stenting the side branch (stent pull-back technique) will limit plaque shifting and reduce the use of additional stents. In addition, proper coverage of the side branch ostium may also reduce 8-month TVR. A case- control design with 100 consecutive patients who underwent drug-eluting stent placement was performed; 55 patients were treated with the stent pull-back technique and 45 patients with a conventional stent technique. Procedural success was 100% for the 2 techniques. The use of additional stents was reduced in the stent pull-back group compared with the conventional stent group (2% vs 18%, p = 0.007). A tendency toward lower ostial miss was also observed in the stent pull-back group (4% vs 13%, p = 0.11). The incidence of in-hospital and 30-day cardiac events was similar between the 2 groups. TVR was lower in the stent pull-back group compared with the conventional group (5% vs 20%; p = 0.03). In conclusion, the stent pull-back technique improves the percutaneous treatment of nonaorto ostial coronary lesions. The technique is associated with a lower use of additional stents and improved clinical outcome, reducing TVR at 8 months of follow-up. Kini AS,Sharma SK. Am J Cardiol 2005;96:1123-8.
- 41. Szabo or ‘tail-wire’ or ‘anchor-wire’ technique TCT 2005. Szabo S et.al. Am J Cardiol 2005;96:212H. (a) proximal end of the anchor wire in the Cx is threaded through the most proximal strut of the crimped LAD stent; (b) stent advanced into lesion until the anchor wire prevents further onward motion. Stent balloon is then inflated at 6-8 atm to allow easy removal of anchor wire; (c) after high-pressure inflation showing satisfactory position.
- 42. Wong P. Catheter Cardiovasc Interv 2008;72:331-4. Proximal flaring of Cypher stent at 4 atm to facilitate threading of anchor wire. The end of the stent is then manually crimped back onto the balloon by gentle squeezing.
- 43. Catheterization and Cardiovascular Interventions 72:331–334 (2008)
- 44. JACC : CARDIOVASCULAR INTERVENTIONS , VOL. 7, N O. 2S, Suppl S, 2014
- 45. JACC : CARDIOVASCULAR INTERVENTIONS , VOL. 7, N O. 2S, Suppl S, 2014
- 46. Author says- “Due to these results, we designed with Hexacath (Paris France) one Stent with a dedicated cell (coming from factory), to simplify the threading of AGW, avoiding balloon puncture or Stent deformation. Our Stent called Titan V, has been successfully implanted in test benches and animal models and currently is under evaluation for CE mark”
- 47. • 257 lesions (78 Szabo technique) • Cross-over occurred in nine (11.7%) Szabo cases vs. no case in the conventional group. EuroIntervention 2010;5:801-808
- 48. Conclusions: The Szabo technique reduces the incidence of angiographic malpositioning in Medina 010 / 001 bifurcations and aorto-ostial lesions, without increasing procedural complications EuroIntervention 2010;5:801-808
- 49. Ostial Pro Stent placement system (For Aorto-ostial lesions only) • The Ostial-Pro (Merit Medical) is a nitinol device with expanded gold-plated feet for treatment of aorta-ostial lesions. • It is advanced into the Toughy-Borst adapter using the supplied introducer to the primary curve in the guide catheter. • The introducer is removed and a 0.014″ coronary wire is advanced distal to the lesion.
- 52. • Fischell and colleagues have reported 30 patients using the Ostial Pro stent placement system in ostial right coronary artery, ostial left main artery, and ostial saphenous vein graft lesions. • They reported a high rate of success with excellent angiographic position. •Fischell TA et al. J Invasive Cardiol. 2009;21(2):53-59.
- 54. Conclusions Establish whether ostial PCI is appropriate (vs. PCI with coverage of SB, or CABG) Guide catheter selection is crucial for aorto-ostial lesions Use optimal, non-overlapped, non-foreshortened angiographic imaging IVUS to assess for proximal or SB disease, degree of calcification,reference diameter and stent expansion Adequate lesion preparation (± adjunctive device use)
- 55. Position proximal stent marker proximal to lesion Minimisation of stent oscillation – breath-hold/shallow breathing,partial pre-inflation Stent ‘draw-back’ or Szabo techniques when conventional positioning is difficult Mandatory high-pressure post-dilatation
- 56. Thank you