
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Similar to Addison's Disease: Rare Adrenal Insufficiency Disorder
Similar to Addison's Disease: Rare Adrenal Insufficiency Disorder (20)
More from promotemedical
More from promotemedical (20)
Recently uploaded
Recently uploaded (20)
Addison's Disease: Rare Adrenal Insufficiency Disorder
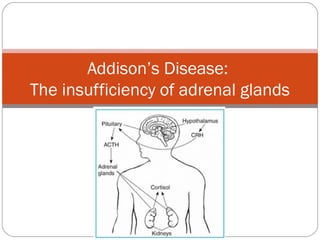
- 1. Addison’s Disease: The insufficiency of adrenal glands
- 2. Introduction Addison’s Disease is a rare and chronic disease that is characterized by adrenal insufficiency There is a decrease in hormones in the adrenal cortex such as glucocorticoids and mineralocorticoids 6-110 cases diagnosed per 100,000 in the world per year. 1.4 million deaths per year around the world. Usually effects 30-50 year-olds, but can be seen in all ages
- 3. History First discovered by Thomas Addison in 1855 First described as an infection of the adrenal gland- most commonly TB. Now instead of infection, its most commonly characterized by an autoimmune destruction of the adrenal glands
- 4. Causes of the Disease Three different causes of the disease Adrenal Dysgenesis: Genetic Causes Imparied Steriodiogensis: Congenital Adrenal Hyperplasia Adrenal Destruction: Autoimmune destruction
- 5. Causes of Disease Adrenal Destruction: Most common type in industrialized world Affects humoral and cell-mediated responses Immune reaction against enzyme 21-hydroxylase, a cytochrome P450 enzyme. Normal functioning 21-hydroxylase catalyzes the addition of an “-OH” on carbon 21 in steroids Addison’s Disease has an enormous amount of autoantibodies attack this enzyme and slowly kill off the adrenal cortex. 82.5% of autoantibodies are adrenal antibodies
- 6. Symptoms Chronic fatigue Muscle Weakness Weight loss, Nausea, Diarrhea Hyperpigmentation Hypercalcemia, Hypoglycemia, Hypoatremia, and Hyperkalemia Esinophilia and Lymphocytosis Metabolic acidosis Addisonian Crisis: Severely low blood pressure and potential coma or death
- 7. How Are the Hormones Affected? When Addison’s disease goes into affect, the Anterior pituitary produces excessive but ineffective amounts of Adrenocorticotropic (ACTH) to the adrenal cortex thus hindering its ability to produce and release hormones (Glucocorticoids and Mineralocorticoids). Since there is no ACTH to stimulate the adrenal cortex to release its hormones, the adrenal cortex can not release hormones to regulate processes in the body.
- 8. Normal Negative Feedback The hypothalamus releases hypothalamic inhibitory or releasing hormones to the anterior pituitary. The anterior pituitary then releases ACTH to the adrenal cortex. The adrenal cortex will then release Glucocorticoids (to raise blood glucose levels or to replenish glucose during or after stressful situations) or Mineralocorticoids (to reabsorb sodium and excrete potassium in order to balance water in the body). When their functions are completed, the target tissues of the hormones will release their own hormones back to the hypothalamus in order to stop the release of hormones to affect the body.
- 9. Normal negative feedback loops Target tissue Hormone of target tissue
- 10. Disrupted Negative Feedback The anterior pituitary releases excessive yet ineffective amounts of ACTH which is supposed to stimulate the adrenal cortex. The adrenal cortex as a result is affected negatively and does not release Glucocorticoids or Mineralocorticoids. Since Glucocorticoids are not produced, glucose cannot be replenished when stressful situations occur. Since Mineralocorticoids are not produced, there is a lack of sodium and water in the body thus leading to severe dehydration. Also, because ACTH exists in excessive yet ineffective amounts, bronzing of the skin occurs because ACTH is linked to melanin production.
- 11. Diagram of disrupted negative feedback Excessive and ineffective amounts of Adrenal cortex hormones are not released
- 12. Diagnosis Determined by low level of adrenal hormone after stimulation with synthetic ACTH hormone tetercosactide Short Test: Compares blood cortisol levels before and after 250 micrograms of tetracosactide if abnormal go to long test Long Test: 1 mg of tetracosactide is administered and blood taken at 1, 4, 8, and 24 hours later
- 13. Current Treatment Replacement corticoidsteroids or fludrocortisone acetate Doses change according to lifestyle, i.e. stress, infection or injury Have to carry emergency injection of hydrocortisone and card/bracelet indentifying their condition
- 14. Clinical Trials Revival of Stem Cells in Addison’s Study Aims to regenerate adrenocorticol steroidogenic cell functions by stimulation proliferation and differentiation of progenitor cells in order to replace damaged adrenal cortex cells
- 15. Conclusion and Future Studies It’s a rare but detrimental disease if left untreated Manageable disease through hormone therapy and helps individuals lead a normal life Future Studies Developing a time release capsule to better mimic the natural fluctuations of the cortisol production