2. CONTENT
• Basic Anatomy
• Definition
• Classification
• Clinical features
• Etiopathogenesis
• Patient evaluation
• Management
• Complications of surgery
3. Skin and subcutaneous tissue
Muscles of protraction
Orbital septum
Orbital fat
Muscles of retraction
Tarsus
Conjunctiva
ANATOMY
4. EYE LID ANATOMY
GROSS DIVISION:
Anterior lamella-skin, orbicularis
oculi
Middle lamella- orbital septum,
orbital fat
Posterior lamella-tarsus,
conjunctiva
5. MAJOR EYELID RETRACTORS
• Upper lid- levator palpebrae superioris muscle with its aponeurosis,
Muller's muscle
• Lower lid- capsulopalpebral fascia and inferior tarsal muscle
6. CANTHAL TENDONS
• cutting, stretching or disinsertion of either of tendons causes horizontal
eyelid laxity
• horizontal eyelid instability is frequently the result of lateral canthal
lengthening
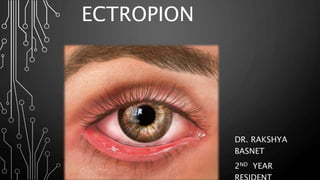
8. KEY FEATURES:
• Eyelid margin and lash drive are turned away from cornea
• Conjunctival surface is exposed, which can lead to keratinisation of
epithelium
• Corneal exposure results in foreign body sensation, corneal dryness
and ulceration
13. CONGENITAL ECTROPION
Rare condition
Due to shortage of skin in eyelids
Usually associated with
• Blepharophimosis syndrome
• Downs syndrome
Euryblepharon : anti-mongoloid slant because of inferiorly displaced
lateral canthal tendon, widened fissures of lateral eyelid with lid
margin not touching globe
14. Senile or involutional
• which is caused by a horizontal lid laxity, lateral and medial canthal
tendon laxity
• lengthening of medial and lateral canthal tendons with ageing
changes
• most common type of ectropion and has a continuous pathological
process that is aggravated by conjunctivitis and epiphora
15. Cicatricial ectropion
• occurs when there is deficiency of anterior lamella tissue (including skin)
on eyelid
• Contracture of skin pulling lid away from globe
• may result from -thermal or chemical injury
-skin conditions or
-contracture by chronic (involutional, mechanical)
ectropian
-surgical trauma
16. Unilateral or bilateral, depending on cause
Unilateral ectropion due to
traumatic scarring
Bilateral ectropion due to
severe dermatitis
19. COMPLICATIONS OF PARALYTIC
ECTROPION
• Exposure keratopathy due to lagophthalmos
• Watering caused by malposition of inferior lacrimal punctum
• Failure of lacrimal pump mechanism
• Increase in tear production from corneal exposure
20. Mechanical ectropion
• occurs when a tractional force is applied to lid by a discrete
lesion
• Caused by-eyelid tumors
-herniated orbital fat
-extravasation of fluid into eyelids
-traction on anterior lamella by eyeglasses
22. • Initial sign of a lower lid ectropion is inferior punctal eversion
this leads to a vicious cycle of secondary events
Eversion of inferior punctum
exposure and drying of punctum
stenosis
Epiphora
excoriation and contracture of skin of lower eyelid that further
exacerbates ectropion
23. Patient tends to continually wipe tears
Eyelid and medial canthal tendon laxity that further exacerbates
lower eyelid ectropion
• If condition is neglected, tarsal conjunctiva becomes exposed and
eventually thickened and keratinized
• Lower lid ectropion often results in a corneal epitheliopathy,
especially in inferior third of cornea
24. It should be directed towards recognition of the ectropion and its
severity
1. Severity of ectropion:
• Mild : The lower punctum is everted
• Moderate : The tarsal conjunctiva is exposed
• Severe : The lower fornix is exposed
2. Extent of ectropion: Medial or lateral or involving the entire lower
eyelid
3. Presence of any traumatic or surgical scar tissue
PATIENT EVALUATION
25. 4. Presence of a horizontal lid laxity
-Eyelid snapback test
-distraction test
5.Medial canthal tendon laxity
-lateral distraction test
6.Lateral canthal tendon laxity
-medial distraction test
27. Grade 0-IV (0 = normal, IV = severe laxity).
• Grade 0 - normal lid that returns to position immediately on release
• Grade I - approximately 2-3 sec
• Grade II - 4-5 sec
• Grade III - >5 sec but does return to position with blinking
• Grade IV - never returns to position and continues to hang down in
frank ectropion after snap-back test
28. (A) A patient with a punctal ectropion. (B) A “Snap” test being performed. (C)
Positive “snap” test: the eyelid fails to return to the globe without a blink
29. ability to pull eyelid more than 6mm from globe
Distraction test
30. Lateral distraction test:
-test for medial canthal tendon laxity
-demonstrated by pulling LL laterally and
observing position of punctum
-normally punctum should not be
displaced >1-2 mm
-mild laxity-punctum reaches limbus
-severe laxity-punctum reaches pupil
31. MEDIAL DISTRACTION TEST
• Test for lateral canthal tendon laxity
• Characterized by a rounded appearance of lateral cathus
• Ability to pull LL medially >2mm
32. • 7. Signs of lower facial nerve palsy as brow ptosis, lid retraction with
incomplete blink, lagophthalmos and absence of nasolabial fold
• 8. Weakness of the preseptal orbicularis oculi is tested by closure of
eyelids
• 9. Examination of corneal sensation is a must
33. Skin shortage?
Abnormal Eyelid
Closure?
Lump in Lid?
Cicatricial
Paralytic
Mechanical
No
No
No
Involutional
Yes
Yes
Yes
MODIFIED ALGORITHM FOR SORTING OUT CAUSE OF
ECTROPION
38. RETROPUNCTAL CAUTERY
• In early stage, in cases of mild medial ectropion with punctal
malposition
Surgical procedure
• Using a disposable cautery device, deep burns are applied to
conjunctiva 3 to 4 mm below punctum
• effect on punctal position is observed and titrated by number of
burns applied and depth of burn
39. MEDIAL ECTROPION WITHOUT HORIZONTAL
LID LAXITY
Medial Spindle Procedure
(Medial Conjunctivoplasty)
Medial conjunctivoplasty
40. MEDIAL ECTROPION WITH HORIZONTAL LID
LAXITY
Medial Spindle Procedure with a Medial Wedge Resection (lazy T
procedure)
• wedge resection is positioned to remove thickened keratinized
conjunctiva
41. -wedge resection is performed just lateral to position of medial
spindle
-wedge resection closure is performed after closure of the
medial spindle
42. MEDIAL CANTHAL RESECTION
Where degree of medial canthal tendon laxity is very
pronounced, however, this can be addressed with a medial
canthal resection procedure
46. Method depends on severity
Severe cases require transposition flaps
or free skin grafts
Mild localized cases are treated by
excision of scar tissue combined
with ‘Z’-plasty
47. Cicatricial ectropion of LOWER LID -3 step procedure
1. Vertical cicatricial traction surgically released
2. Eyelid is horizontally tightened with lateral tarsal strip procedure
3. Anterior lamella is vertically lengthened via mid-face lift or full
thickness skin grafts
Cicatricial ectropion of UPPER LID -1 step procedure
1. Release of traction & augmentation of vertically shortened
anterior lamella with full thickness skin graft
49. 1.TEMPORARY TREATMENT
• Lubrication with tear substitutes during day
• Botulinum toxin injection
• Temporary tarsorrhaphy in patients with poor Bell’s
phenomenon
Temporary
tarsorrhaphy
54. BIBLIOGRAPHY
• AAO series: Orbit, Eyelid and Lacrimal system
• Jack J kanski, Brad Bowling, Clinical Ophthalmology
• Yanoff and Duker Ophthalmology
• Anatomy & Physiology-A.K. Khurana
• Wolff’s anatomy
• Richard Collins book on eyelid surgery