Liver Abscess and Hydatid Cyst, Surgery
•Download as PPTX, PDF•
18 likes•1,115 views

Liver amebic and pyogenic abscess, hydatid cyst, surgical management, sabiston textbook

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Liver Abscess and Hydatid Cyst, Surgery
Similar to Liver Abscess and Hydatid Cyst, Surgery (20)
More from GunJee Gj
More from GunJee Gj (20)
Recently uploaded
Recently uploaded (20)
Liver Abscess and Hydatid Cyst, Surgery
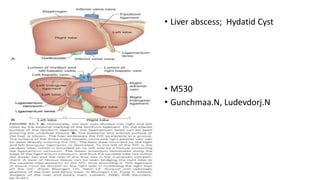
- 1. • Liver abscess; Hydatid Cyst • M530 • Gunchmaa.N, Ludevdorj.N
- 5. Epidemiology • Patients in their 50s or 60s • Often related to biliary tract disease • Cryptogenic in nature (uncertain in origin)
- 6. Pathogenesis • An inoculum of bacteria exceeds the livers ability to clear it. • Tissue invasion • Neutrophil infiltration • Abscess formation
- 7. Biliary tree • Stone or malignant disease • Biliary obstruction • Bile stasis • Bacterial colonization • Ascends to liver • Ascending suppurative cholangitis
- 8. Portal vein • Ascending portal vein infection – pyelophlebitis • Diverticulitis, appendicitis, pancreatitis, IBD etc • Malignant disease
- 9. Hepatic artery • Any systemic infection • Altered immune response • Direct infection extension
- 10. Other causes • Necrotic liver: • Trauma • Hepatic artery embolization • Thermal ablative procedures
- 11. Pathology • 75% right hemiliver • 20% left hemiliver • 5% caudate lobe • Mostly solitary • 1 mm – 4 cm • Multiloculated or in single cavity
- 12. Microbiology • Either polymicrobial or single organism • Escherichia coli • Klebsiella pneumoniae • Staphylococcus aureus • Enterococcus sp.
- 13. Clinical features • Fever • Chills • Jaundice • RUQ pain • Tenderness to palpation • Hepatomegaly • Acute or chronic
- 14. Complication • If diaphragm is involved, cough or dyspnea • Peritonitis secondary to rupture • Rupture into pleural space or pericardium • Endogenous endophthalmitis (Klebsiella)
- 15. Lab findings • Leukocytosis • Anemia • LFT abnormality • ALP elevated /80%/ • Total bilirubin elevated /20-50%/ • Transaminases increase /60%/ • Hypoalbuminemia, increased PT
- 16. Radiology • Chest X-ray Atelectasis Right pleural effusion Elevated right hemidiaphragm • Plain abdominal X-ray - Air fluid levels - Portal venous gas
- 17. Radiology • Ultrasound – round or oval, less echogenic than surrounding liver • CT – lesions are of lower attenuation than surrounding liver, multiple small abscesses • Both are useful in diagnosing intra-abdominal diseases
- 19. Differential diagnosis • Amebic abscess • Echinococcal cyst
- 20. Treatment • Immediate broad spectrum IV antibiotics /2 weeks</ • Combination of ampicillin, aminoglycosides, metronidazole • Aspiration, send for culture. • Percutaneous catheter drainage • Contraindications: ascites, coagulopathy, proximity to vital structures • If larger than 5 cm, surgery is better • Liver resection if destruction is severe
- 21. Amebic Abscess
- 22. Epidemiology • Largely a disease in tropical or developing countries • Less than 50% are symptomatic • Mostly Hispanic men • 20-40 age • Socioeconomic status • Alcohol consumption • Immunosuppression • Travel history
- 23. Pathogenesis • E.histolytica is a protozoan that exists as trophozoite or cyst • Fecal-oral route • When ingested, cysts aren’t degraded in stomach • Trophozoite released • Invades colon mucosa • Enzymatic cellular hydrolysis
- 24. Pathogenesis • Localized necrosis • Cavity forms • It contains proteinaceous debris • Surrounded by rim of trophozoites • Rapid IgA release
- 25. Pathology • Cavity full of blood, liquefied liver tissue • The fluid is odorless • Glisson capsule resistant to hydrolysis • Early stage, ill-defined • Right hemiliver
- 26. Clinical features • Last from days to 4 weeks • Fever • Chills • RUQ pain and tenderness • Hepatomegaly • Constant, dull abdominal pain • Diarrhea • Anorexia • Jaundice
- 27. Clinical features • Acute <10 days • High fevers, chills, abdominal tenderness • Multiple lesions usually • Chronic > 2 weeks • Single right-sided lesion • Response is similar in both groups
- 28. Lab findings • Mild to moderate leukocytosis with no eosinophilia • Anemia • LFT abnormality • Elevated PT-INR • Enzyme immunoassay • Detection kit
- 29. Radiology • Plain chest x-ray: elevated right hemidiaphragm, pleural effusion, atelectasis • Ultrasound: Round lesions, liver capsule, without significant rim echoes. Contents are hypoechogenic, nonhomogenous • CT: more sensitive • Nuclear studies: to differentiate from pyogenic abscess. No leukocytes, does not light up
- 31. Differential diagnosis • Viral hepatitis • Echinococcal disease • Cholangitis • Cholecystitis • Appendicitis • Liver tumor • Pyogenic abscess
- 32. Treatment • Metronidazole 750 mg orally, three times daily, 10 days • Emetine hydrochloride • Chloroquine • After liver abscess is treated, iodoquinol, paromomycin, diloxanide furoate to treat carrier state • If failure of metronidazole in 3-5 days, diagnostic aspiration • Larger than 5 cm, in left side – aspiration • Radiologic resolution 3-9 months
- 33. Hydatid Cyst
- 34. • Hydatid disease or echinococcosis is a zoonosis that is common worldwide because the dog is a definitive host. • Human contract the disease from dogs, but there is no human to human transmission
- 35. • 3 species that cause hydatid cyst: • Echinococcus granulosus • Echinococcus multilocularis • Echinococcus ligartus • Humans are end stage to the parasite.
- 36. • In the human duodenum, the parasitic embryo releases an oncosphere containing hooklets that penetrate the mucosa, allowing access to the bloodstream. • In the blood, it can reaches the liver or lungs, where the parasite develops its larval stage
- 37. • 3 weeks after infection, a visible hydatid cyst develops, which then slowly grows in a spherical manner.
- 38. • The cyst wall itself has 2 layers, an outer gelatinous membrane (ectocyst) and an inner germinal membrane (endocyst). • Brood capsules are small, intracystic cellular masses in which future worm heads develop into scoleces. In a definitive host, the scoleces develops into an adult tapeworm.
- 39. Hydatid cysts can die with: • degeneration of the membranes • Development of cystic vacuoles • Calcification of the wall • Calcification of a hydatid cyst, however, doesn’t always imply that the cyst is dead
- 40. • Hydatic cysts are diagnosed in equal numbers of en and woman at an average age of about 45 years. • Approximately 75% of hydatid cysts are located in the right liver and are solitary
- 41. • The clinical presentation of a hydatid cyst is largely asymptomatic until complications occur. • Dyspepsia • Abdominal pain • Vomiting • Hepatomegaly are the most common symptoms.
- 42. • Jaundice and fever are each present in approximately 8% of patients. • Bacterial super infection of a hydatid cyst can occur and be manifested like a pyogenic abscess
- 43. • Rupture of the cyst into the biliary tree or bronchial tree or free rupture into the peritoneal , pleural, or pericardial cavities can occur.
- 44. Diagnosis • Serologic tests are available to evaluate antibody response, but all are plagued by low sensitivity and specifity • Ultrasound is more common, but it depends on the stage of the cyst at the time of examination
- 45. • Simple hydatid cyst is well circumscribed with budding signs on the cyst membrane • May contain free floating hyperechogenic hydatid sand • A rosette appearance is seen when daughter cysts are present
- 46. • Cyst can be filled with an amorphous mass, which can be diagnostically misleading • Calcification in the wall of the cyst is highly suggestive of hydatid disease
- 48. • Similar findings are seen on CT or MRI scans • In patients with suspected biliary involvement, ERCP or percutaneous transhepatic cholangiography may neccesary
- 49. Treatment • Primarily surgical • Most cyst should be treated • But in older patients with small, asymptomatic, densely calcified cysts, conservative management ( drainage nad evacuation) is appropriate.
- 50. • Epinephrine and steroids taken by anesthesiologist • Packing off the abdomen is important because rupture can result in anaphylaxis and diffuse seeding
- 51. • Then cyst ih aspirated through a closed suctionsystem and flushed with a scolicidal agent (hypertonic saline)
- 52. • The cyst is then unroofed which can then be followed by a number of possibilities, including • excision ( or pericystectomy) • Marsupialization procedures • Leaving the cyst open • Drainage of the cyst • Omentoplasty • Partial hepatectomy
- 53. • Pericystectomy or formal partial hepatectomy can also be performed without entering thy cyst.
- 54. • Simple suture repair is often sufficient, but major biliary repairs, approaches through the common bile duct, or postoperative ERCP may be neccesary • Recurrence rates after surgical treatment is generally 5% or less
- 55. • Preoperative treatment my decrease the risk of spillage. • Albendazole or mebendazole is effective with E.granulosus infection, but cyst appearance occurs 50% of patients • Medical treatment without resection or drainage should be considered only for widely diseminated disese or poor surgical candidate
- 56. Thank you!
Editor's Notes
- No significant difference in age, gender and ethnicity.
- Poly – cholangitis, pyelophlebitis. Single – systemic infections
- Important because of difference in treatment.
- Advantage is avoidance of general anesthesia, laparotomy, simple.
- Human contact with carrier, contaminated water food. Lyses through cell adhesion, release of enzymes, resulting in necrosis
- Can calcify
- Typically less than 10 days. Can compress biliary tree
- LFT – albumin, PT- INR, ALP, AST, bilirubin