High Profile Call Girls Jaipur Vani 8445551418 Independent Escort Service Jaipur
Cvp line
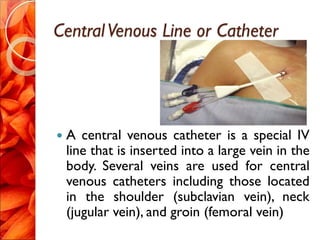
1. CentralVenous Line or Catheter
A central venous catheter is a special IV
line that is inserted into a large vein in the
body. Several veins are used for central
venous catheters including those located
in the shoulder (subclavian vein), neck
(jugular vein), and groin (femoral vein)
5. In some patients, a central venous
catheter may be inserted into the
elbow vein (anticubital vein) and
advanced into the subclavian vein.
6.
7. PURPOSE
These special IVs are used when the
patient either does not have adequate
veins in the arms or needs special
medications and/or nutrition that cannot
be given through the smaller arm veins.
Serve as a guide of fluid balance in
critically ill patients.
Determine the function of the right side
of the heart
8. complication
Bleeding and infection are complications
associated with IV catheters. As previously
mentioned, collapse of a lung is a rare
complication of central venous catheters.
If this occurs, a chest tube (thoracostomy
tube) may be required to re-expand the
lung.
9. Arterial puncture, cardiac puncture
Pneumothorax, Hemomothorax
Air emboli,Thrombosis
Cardiac temponade
Cardiac arrhythmias
Carotid Artery Puncture
Perforation of SVC or R.Atrium/Ventricle
Pleural Effusion
10. NURSES ROLE
Monitor for the signs of complications.
Assess for patency of the CVP line.
Sterile dressing should be done to
prevent infection( CVP care per the
hospital protocol)
The length of the indwelling catheter
should be recorded and regularly
monitored.
11. ICP monitor
ICU patients who have sustained head
trauma, brain hemorrhage, brain surgery,
or conditions in which the brain may
swell might require intracranial pressure
monitoring.
12. PURPOSE
The purpose of ICP monitoring is to
continuously measure the pressure
surrounding the brain. If the pressure
surrounding the brain gets too high, it can
cause decreased blood flow to the brain
and potentially lead to brain damage.
13. The ICP monitor is usually inserted by a
neurosurgeon while the patient is in the
ICU or operating room. After using
numbing medicine (local anesthetics), the
neurosurgeon makes a skin incision and
inserts the ICP monitor into the brain
through a very small hole created in the
skull.
14. The ICP monitor is usually inserted in the
left or right top-front part of the brain.
Some ICP monitors can drain spinal fluid if
necessary.
17. PULSE OXIMETER
A pulse oximeter is the device that
measures and displays the oxygen arterial
saturation. The study is called pulse
oxymetry.
The pulse oximeter is a small device that
has to be in contact with the skin to detect
the oxygen saturation.
18. The device is usually place on the
patient's finger, earlobe, toe or nose. The
pulse oximeter gives off light that
determines the oxygen saturation of the
blood.
19. Breathing Machine (Mechanical
Ventilator
A breathing machine
helps the patient
breathe. It is designed
to help patients who
cannot breathe
adequately on their
own. The breathing
machine does not fix
any problems of the
lungs.
20. It is a device that simply pushes air and
oxygen into the lungs and withdraws
carbon dioxide from the lungs. The lungs
must function in order for the breathing
machine to be effective.
21. PURPOSE
A breathing machine is
used whenever a
patient cannot breathe
without assistance.
Doctors, nurses and
respiratory therapists
all work to make sure
a breathing machine is
not used any longer
than necessary.
22. The goal when a breathing machine is
first used is to get the patient to be able
to breathe on their own, so that the
breathing machine can be removed.
23. complications
Patients who require breathing machine
support are at increased risk to develop
pneumonia. Occasionally, patients may
develop a collapsed lung. Both of these
complications require treatment
24. NURSES ROLE
Promoting effective airway clearance.
preventing trauma and infection.
Check
Ventilator functioning properly
Blockage of air passage
Too much sputum, secretions
When sedation drugs are used
ABG, hypoxia
25. b. Suction periodically as per need
c. Change the mode setup as adviced.
d. Give sedatives as adviced.
26. INFUSION PUMP
An intravenous (IV) infusion pump is a
machine that carefully controls the rate at
which IV fluids and/or IV medications are
given.
27. PURPOSE
Under some circumstances, the rate at
which IV fluids and/or IV medications are
given needs to be closely controlled.
28. These pumps are very reliable. Mechanical
problems are possible, but very rare. If the
IV infusion pump does not work correctly,
an alarm will sound.
29. NURSES ROLE
Using aseptic technique and universal
precautions, iv infusion should be set.
Set the flow rate as prescribed calculating
the amount of fluid.
Observe for the signs of infiltration or
other complications such as
thrombophlebitis. Fluid or electrolyte
overload and embolism before
administration.
30. Resuscitation Cart (Crash Cart)
The resuscitation cart
contains all of the
equipment and
medications needed
for advanced life
support and CPR
(cardiopulmonary
resuscitation).
31. purpose
This emergency equipment is used only if
the patient's heart or lungs stop working.
The cart is brought to the patient's
bedside when the patient's heart or lungs
are failing or have failed.
32. NURSES ROLE
Keep the resuscitation cart ready all the
time.
Check the devices and ensure that the
devices are kept in charging.
Check for the emergency (life saving)
medication for their expiry date.
33. DEFIBRILLATOR
A defibrillator is a device that is designed
to pass electrical current through a
patient’s heart. The passing of electrical
current through the heart is called
defibrillation. A defibrillation is done
through pads placed on the patient’s chest.
34. purpose
A defibrillation is used to restore a
patient’s heart rhythm to normal.
Abnormal heart rhythms may be treated
with medications while other rhythms
need to be treated with defibrillation.
35. Life threatening heart rhythms need
defibrillation immediately while other heart
rhythms may be defibrillated in a scheduled
fashion.
Defibrillation may be done using the manual
defibrillator or the automatic external
defibrillator (AED).
36. Complication
The defibrillator pads may cause a skin
irritation and leave a temporary redden
area where they contacted the chest.
Unfortunately defibrillation does not
always return the patient’s heart rhythm
back to normal.
37. NURSES ROLE
Keep the patient in comfortable position
and obtain 12 lead ECG.
Give the patient 100 % oxygen by
inhalation.
Apply electrode paste on the DC paddle,
rub it and apply the paste at the patient’s
chest in the second intercostal space at the
right side of breast line and at the apex of
the heart.
38. TURN OFF the oxygen to the patient as a
spark from paddle could blow the oxygen
on the fire.
Be sure to say “ ALL CLEAR”. No one
should touch the patient or the bed during
cardioversion.
Check the rhythm on ECG monitor.
Keep the patient in comfortable position
and give 100% oxygen by inhalation.
39. Report and record the procedure and
clean the paddle area with spirit swab.
Keep the difibrilator on continue electrical
charging.
40. MAINTENANCE OF ICU
EQUIPMENTS
Since ICU equipment is used continuously
on critically ill patients, it is essential that
equipment be properly maintained,
particularly devices that are used for life
support and resuscitation.
41. Contd…
Staff in the ICU should perform daily checks
on equipment and inform biomedical
engineering staff when equipment needs
maintenance, repair, or replacement.
For mechanically complex devices, service
and preventive maintenance contracts are
available from the manufacturer or third-
party servicing companies, and should be
kept current at all times.
42. Health care team roles
Equipment in the ICU is used by a team
specialized in their use. The team usually
comprises a critical care attending
physician (also called an intensivist), critical
care nurses, an infectious disease team,
critical care respiratory therapists,
pharmacologists, physical therapists, and
dietitians.
43. Radiologic technologists perform mobile x
ray examinations (bedside radiography).
Either nurses or clinical laboratory
personnel perform point-of-care blood
analysis. Equipment in the ICU is
maintained and repaired by hospital
biomedical engineering staff and/or the
equipment manufacturer.
45. INTRODUCTION
Intensive care unit (ICU) equipment
includes patient monitoring, respiratory
and cardiac support, pain management ,
emergency resuscitation devices, and
other life support equipment designed
to care for patients who have a critical
or life-threatening illness, thereby
requiring 24-hour care and monitoring.
45
46. PURPOSE
An ICU may be designed and equipped to
provide care to patients with a range of
conditions, or it may be designed and
equipped to provide specialized care to
patients with specific conditions.
46
47. ICU BED
Comfy ICU Bed (7 function) with
electrically operated back rest tilting 0-80°,
knee rest tilting 0-35°, trendelenburg tilting
0-20°, Reverse trendelenburg tilting 0-20°,
mattress base tilting to the left up to 40°,
tilting to the right up to 40°.
Size: 2155 x 940 x 630 / 1030 mm.
All functions controlled with Power Device
.
47
48. Contd….
Four easy lifting guardrails (2 on each
side), which are safe and reliable, and can
be fixed upward and downward.
Easy to operate built-in Control Panel on
both sides of guard rails.
48
49. Contd….
Foot Step Control Panel under the bed
frame.
Removable & interchangeable high quality
ABS engineering plastic head panel and
foot panel.
Head panel and foot panel equipped with
safety lock and roller bumpers.
49
50. Contd…
Epoxy coated mild steel frame work and
4 section perforated top.
125mm dia noiseless castors with
simultaneous braking system which locks
/ unlocks 2 castors with single pedal
press.
Provision for I.V. Rod on both sides of the
bed.
50
55. TYPES OF DEVICES
Intensive care unit equipment includes:
Patient monitoring devices
Life support and emergency
resuscitation devices, and
Diagnostic devices.
55
63. 3.CARDIAC PACING
Cardiac Pacing is
the repetitive
delivery of very
low electrical
energies to the
heart to initiate
and maintain
cardiac rhythm.
63
67. WHAT IS CENTRALVENOUS
PRESSURE
• Is the pressure within the superior vena cava or the
right atrium
• The CVP catheter is an important tool used to assess
right ventricular function and systemic fluid status.
• Helps to determine the venous return and
intravascular volume of the right atrium.
• The normal value is 5-10cm H2O
68. Purposes of CVP
measurement
To serve as a guide of fluid balance in critically ill
patients
To estimate the circulating blood volume
To determine the function of the right side of
the heart
To assist in monitoring circulatory failure
70. WHAT IS A CENTRAL LINE
It is a catheter that
provides venous
access via the superior
vena cava or right
atrium
71. CENTRAL LINES
• purposes of CVP lines are:
-Fluid resuscitation
– Parenteral feeding
– Measurement of central venous pressure
– Poor venous access
– For transfusion
– For chemotherapy
– To give ionotropes
– For sampling blood
72. INDICATION OF CVC
i) Major operative procedures involving large fluid shifts
and / or blood loss
ii) Intravascular volume assessment when urine output is
less or not present(e.g renal failure)
iii) Major trauma
iv) Surgical procedures with a high risk of air embolism,
such as craniotomies.
v)To aspirate intracardiac air.
vi) Special Uses as insertion of PA catheters
,haemodialysis/ plasmapheresis
vii) Hypovolemic shock
viii) Myocardial dysfunction
73. COMMON SITES OF CVP LINE
INSERTION
CENTRAL SITE
Right internal jugular
Left internal jugular
Right subclavian
Left subclavian
PERIPHERALLY
INSERTED CENTRAL
CATHETERS (PICC)
antecubital veins
basilic vein
Cephalic vein
Femoral artery
77. INTERNAL JUGULAR
10-12 cm
Better for CVC
Easy to pass, less chance
of pneumothorax, in direct
contact with right atrium
Difficult to maintain as it is
mobile and chance of
infection
Commonly done in
BPKIHS,ICU.
78.
79. SUBCLAVIAN
• 8-10cm
• In hypovolemia
subclavian remains
dilated so best route
• Less mobile
• Can be kept for larger
period (6 months, 3
months for
chemotherapy)
80. PERIPHERAL ROUTE
• Easy to cannulate,
less chance of severe
complication, no
chance of
pneumothorax
• Long catheter is
required so flow rate
of IV fluids and drugs
is slow.
81. TYPES OF CENTRAL LINE
SINGLE LUMEN
DOUBLE LUMEN
TRIPLE LUMEN
QUADRUPLE LUMEN
82. Right position to keep the tip
of catheter
At the junction of
superior venacava
and right atrium.
Seldinger technique
is used in CVP Cannulation
83. Patient is kept in trendenleberg position
The cannula with stylet is inserted at the tip of
triangle formed by 2 heads of sternomatoid and
clavicle.The direction of needle is slightly lateral
Once internal jugular is punctured stylet is
removed and guide wire is passed and catheter is
inserted.
84. Head turned to left,
Trendelenberg
position, two heads
of
sternocleidomastoid
85.
86.
87. Post-Catheter Placement
Aspirate blood from each port
Flush with saline or sterile water
Secure catheter with sutures
Cover with sterile dressing (tega-derm)
Obtain chest x-ray for IJ and SC lines
Write a procedure note
89. Injection Cap
Pigtail or
lumen luer
connector
Individual lumens or pigtails
Catheter juncture
hub
Pigtail or
lumen slide
clamp
90. METHODS OF CVP
MONITORING
• There are two methods of CVP monitoring
–manometer system: enables intermittent
readings and is less accurate than the
transducer system
–transducer system: enables continuous
readings which are displayed on a monitor.
91. CVP MONITORING USING MANOMETER
• The CVP catheter is connected to water filled
water manometer column via a 3 way cannula.
• Find out the zero reference point(phlebostatic axis)
from midaxillary line at 4th intercoastal space.
• Flush the CVP line
• Flush the manometer
• Close the heparin flush line and open CVP line and
manometer
• Where the fluid get stabilised ,count from the zero
reference
92.
93. MONITORINGWITHTRANSDUCERS
• Transducers enable the pressure readings
from invasive monitoring to be displayed on a
monitor.
• To maintain patency of the cannula a bag of
normal saline or heparinised saline should be
connected to the transducer tubing and kept
under continuous pressure of 300mmHg thus
facilitating a continuous flush of 3mls/hr
94. PROCEDURE FOR CVP
MEASUREMENT USING A
TRANSDUCER
explain the procedure to the patient
ensure the line is patent
position the patient supine (if possible) and align the
transducer with the mid axilla (level with the right
atrium)
zero the monitor
observe the CVP trace
document the reading and report any changes or
abnormalities
95. THE CVPWAVEFORM
The CVP waveform reflects
changes in right atrial
pressure during the cardiac
cycle
Mechanical events during the
cardiac cycle are responsible
for the sequence of waves
seen in a typical CVP trace.
The CVP waveform consists
of five phasic events, three
peaks (a, c, v) and two
descents (x, y)
96. The normal CVP waveform
1. The ‘a’ wave : right atrial
contraction
2. The ‘c’ wave : ventricular
contraction.
3. X descent: Decrease in the
pressure within the RA
with right ventricular
ejection.
4. V wave : Filling of RA during
late ventricular systole
5. The Y descent :Empyting of
RA into the RV during early
diastole.
99. CVP is elevated by :
◦ Overhydration, Hypervolemia which
increases venous return
◦ Heart failure or PA stenosis,
◦ forced exhalation
◦ Pneumothorax
◦ Heart failure
◦ Pleural effusion
◦ Decreased cardiac output
◦ Cardiac tamponade
100. CVP decreases with:
Hypovolemia, hypovolemic shock from
hemorrhage, fluid shift, dehydration
◦ Deep inhalation
101. Contraindications
Infection at the site of insertion
Coagulopathies
Newly inserted pacemaker wires
Presence of carotid disease
Recent cannulation of the internal jugular vein
Contra lateral diaphragmatic dysfunction
Thyromegaly or prior neck surgery:
102. MANAGEMENT OF A PATIENT WITH A CVP LINE
Monitor the patient for signs of complications
Label CVP lines with drugs/fluids etc. being
infused in order to minimise the risk of
accidental bolus injection
If not in use, flush the cannula regularly to help
prevent thrombosis.
Sterile dressing should be done to prevent
infection.
103. Cont…
Ensure all connections are secure to prevent
dislodgement, introduction of infection and air
emboli
Observe the insertion site frequently for signs of
infection.
The length of the indwelling catheter should be
recorded and regularly monitored.
CVP lines should be removed when clinically
indicated
104. Nursing and Catheter Care
Equipment:
Sterile dressing tray
Sterile cotton-tipped applicators
Cleansing swabs
Cleansing solution (Use of commercially available
chlorhexidine impregnated sponge dressing may be used)
Wound adhesive tapes (Steri Strips)
Clear tape
Non-sterile gloves
Sterile gloves
105. Procedure:
•Wash hands.
•Prepare tray and supplies.
•Put on non-sterile gloves.
•Remove dressing.
•Remove gloves.
•Wash hands.
•Put on sterile gloves.
•Remove steri strips and wings using forceps.
•Inspect the catheter site. If there is any sign of infection, swab
the site for C&S and notify the physician.
•Cleanse around and under catheter using cotton-tipped
applicators.
106. Cont...
Cleanse the insertion site starting at the catheter and
working outwards in a circular motion to a radius of 10
cm. Avoid crossing over the catheter. Repeat twice using
a new swab each time.
Cleanse the top and underside of the catheter, starting
at the exit site.Allow to dry.
Cleanse wings with cleansing solution. Allow to dry
prior to replacing.
107. Re-apply wings by squeezing the wing together so that it
splits open. Place wings on catheter. Ensure that catheter is
within the channel under the wings. Cleanse catheter and
insertion site with applicators/gauze soaked in cleansing
solution.
Apply steri strips to secure wings. Tuck steri strips under
wings and catheter so that catheter is supported off skin, but
secure.
Apply sterile dressing to site. Create a loose loop so that the
catheter is not twisted or kinked under the dressing
108. COMPLICATIONS FOLLOWING CVP
LINE INSERTION
Malposition of the catheter
Haematoma
Arterial puncture, cardiac puncture
Pneumothorax, Hemomothorax
Haemorrhage
Air emboli,Thrombosis
Cardiac temponade
Cardiac arrhythmias
.
112. PCWP
Pulmonary capillary wedge pressure
(PCWP) provides an indirect estimate of
left atrial pressure (LAP).
Normal PCWP 8-10mm Hg
113. How is it measured?
PCWP is measured by inserting balloon-tipped,
multi-lumen catheter (Swan-Ganz catheter)
into a peripheral vein, then advancing the
catheter into the right atrium, right ventricle,
pulmonary artery, and then into a branch of the
pulmonary artery.
Just behind the tip of the catheter is a small
balloon that can be inflated with air (~1 cc). The
catheter has one opening (port) at the tip (distal
to the balloon) and a second port several
centimeters proximal to the balloon. These ports
are connected to pressure transducers.
114. Cont…
• The balloon is then inflated, which occludes
the branch of the pulmonary artery. The
pressure rapidly falls and reaches a stable
lower value that is very similar to left atrial
pressure (normally about 8-10 mmHg). The
balloon is then deflated.
115.
116. Why is it measured?
• to diagnose the severity of left ventricular failure
• to quantify the degree of mitral valve stenosis. Aortic
valve stenosis and regurgitation, and mitral regurgitation
also elevate LAP(above 20 mmHg) causing pulmonary
edema which is a life-threatening condition.
• PCWP is also useful in evaluating blood volume status
when fluids are administered during hypovloemic shock.
117. Cont…
It is necessary to measure when evaluating
pulmonary hypertension(due to increase in
pulmonary vascular resistance)
To titrate the dose of diuretic drugs and other drugs
that are used to reduce pulmonary venous and
capillary pressure, and reduce the pulmonary edema.
118. Indications For PCWP
Monitoring:
A. Cardiac cause:
Recent MI
Complications of MI eg. MR,VSD, ventricular aneurysm.
Combined lesions eg. CAD+MR or CAD+AS
B. Non-cardiac situations:
Shock of any cause
Severe pulmonary disease
Complicated surgical procedure
Massive trauma
Hepatic transplantation
123. GCS
• Glasgow Coma Scale or GCS, sometimes
also known as the Glasgow Coma Score is a
neurological scale which aims to give a reliable,
objective way of recording the conscious state of
a person, for initial as well as continuing
assessment.
• The scale was published in 1974 by Graham
Teasdale and Bryan J. Jennett, professors of
neurosurgery at the University of Glasgow.
124. Components of the GCS
• There are three components to the GCS:
• Best eye opening
• Best motor response
• Best verbal response
Each is evaluated independently of the other two
components.
ALWAYS SCORE THE BEST RESPONSE
FORTHE PATIENT
125. Cont…
The three values separately as well as their
sum are considered. The lowest possible
GCS (the sum) is 3 (deep coma or death),
while the highest is 15 (fully awake
person).
126. • Scoring
– Eye Opening
• Spontaneous: 4
• To speech: 3
• To pain: 2
• No Response: 1
– Best Verbal Response
• Oriented (Infant coos or babbles): 5
• Confused (Infant irritable cries): 4
• Inappropriate words (Infant Cries to pain): 3
• Incomprehensible sounds (Infant Moans to pain): 2
• No Response: 1
– Best Motor Response
• Obeys (Infant moves spontaneous/purposefully): 6
• Localizes (infant withdraws to touch): 5
• Withdraws to pain: 4
• Abnormal Flexion to pain (Decorticate): 3
• Extensor Response to pain (Decerebrate): 2
• No Response: 1
127. Best eye response (E)
If there is damage to the occulomotor nerve from trauma, the
patient may not be able to open his or her eye. :
1=No eye opening (regardless of any stimuli)
2=Eye opening in response to pain. (Patient responds to
pressure on the patient’s fingernailbed supraorbital and sternal
pressure)
3=Eye opening to speech. (either spoken or shouted verbal
response)
4=Eyes opening spontaneously (when a person approaches
bedside)
128. BestVerbal Response (5 - 1)
Verbal response assesses consciousness by
determining whether a person is aware of
him/herself and the environment.
129. Best verbal response (V)
1=No verbal response
2=Incomprehensible sounds.
3=Inappropriate words
4=Confused.
5=Oriented.
130. Orientation
There are six specific questions in the original
GCS
• What is your name?
• Where are you?
• Why are you here?
• What month are we in?
• What year are we in?
• What season are we in?
131. Confusion (4)
A patient may be able to hold a conversation
with the observer but responses are
inappropriate or disoriented.
132. Inappropriate Speech (3)
Does not carry on conversation, poor
attention span, uses inappropriate words
and phrases.
Random/confused/repetitive.
133. Incomprehensible Speech (2)
Patients are less aware of their environment
and their verbal response is in the form of
incomprehensible sounds.
• Moan or cry
• The observer may now have to use both a
painful and verbal stimulus to get a
response.
134. Best Motor Response (6 – 1)
6= Obeys commands
5= Localises to pain
4=Withdraws from pain
3= Abnormal flexion
2= Extension
1= No response
135. Obeys Commands (6)
Patients are aware of their environment, have
understood the observer's instructions, and are
to carry them out.
• Examples of possible commands are 'lift up your
arms' or 'hold up your thumb'.
• If patients are asked to 'squeeze my hands', they
must also be asked to release their grip.
136. Localises to Pain (5)
• This is a response to a central painful stimulus.
• It involves the higher centres of the brain, the
cerebral hemispheres or cerebrum.
• usually a motor response such as moving an
arm towards the source of the pain in order
to remove it and stop the pain from
continuing pain stimuli
137. Withdraws from pain (4)
Patients flex or bend their arm towards
the source of the pain, but do not actually
localise or try to remove the source of the
pain
138. Abnormal Flexion (3)
• Patients flex or bend the arm at the elbow
and rotate the wrist, resulting in a spastic
posture in response to a central painful
stimulus.
• It is an abnormal response and indicates
severe cerebral damage and an interruption of
nerve pathways from the brain's cortex to the
spine.
140. Extension (2)
• In response to a central painful stimulus,
patients will extend or straighten an arm at
the elbow, or may rotate the arm inwards.
• Abnormal response due to damage to the
brain stem by which information to and from
the cerebrum are not tranmitted.
142. Severe, with GCS ≤ 8 - that is also a
generally accepted definition of a coma
Moderate, GCS 9 - 12
Minor, GCS ≥ 13.
143. • The motor component of the GCS score is a
powerful predictor of outcome and contains
most of the predictive power of the score.
• There are two circumstances in which the
motor-only model is unreliable: in patients with
pharmacologic (therapeutic) paralysis and in
patients with traumatic paralysis (i.e., high spinal
cord injuries). In these cases, the motor score is
simply not a measure of consciousness and
cannot be used as one.
144. Others methods:
AVPU Scale
A-alertness
V-verbal response
P- response to pain
U-unresponsive
3 GCS components
3-point scores
a) simplified verbal score: oriented=2, confused conversation=1,
inappropriate words or less=0
b) simplified motor score: obeys commands=2, localizes pain=1,
withdrawal to pain or less=0).
We then compared the test performance of each of these 5 to the total
GCS score using a priori thresholds for clinically important differences.