VarSeq 2.6.0: Advancing Pharmacogenomics and Genomic Analysis
Final pediatric emergency ultrasonography
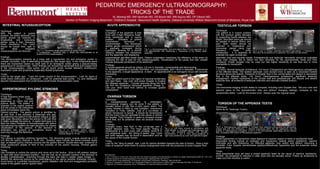
1. PEDIATRIC EMERGENCY ULTRASONOGRAPHY:
TRICKS OF THE TRADE
KL Moreng MD, RM VanHulle MD, DA Bloom MD, MR Aquino MD, DP Gibson MD,
Section of Pediatric Imaging,Beaumont Children’s Hospital , Beaumont Health Systems, Oakland University William Beaumont School of Medicine, Royal Oak, MI
INTESTINAL INTUSSUSCEPTION ACUTE APPENDICITIS TESTICULAR TORSION
Technique: Technique: Technique:
With the patient in supine Evaluation of the appendix is best The patient is in supine position
position, the entire abdomen and done with a high frequency linear- with the scrotum gently elevated
pelvis should be scanned in array transducer and in supine by supporting towels between the
longitudinal and transverse position. Utilization of graded thighs. Abundant warm gel should
planes using a high frequency compression technique is be applied to reduce friction and
linear transducer. The colon recommended. The transducer pain. Both testes should be
should be traced from right to a applies gentle compression which a b c scanned in longitudinal and
left. Most idiopathic
b c is gradually increased during Fig 3: a. Noncompressible, fluid and debris filled 10 mm appendix. b. 8 transverse planes using high a b c
intussusceptions are ileocolic. Fig 1. a. Transverse target appearance at splenic flexure. expiration, allowing for a shorter mm appendicolith with shadowing c. Hyperemia of the dilated distal frequency, linear array Fig 5. a. and b. Twisted spermatic cord above right testicle. c. Presence of
b. Longitudinal – sandwich sign. c. Blood flow demonstrated to all distance between the transducer appendix. transducers . It is essential to flow within the left testicle but no significant flow within the right testicle.
portions of the intussusception. and the appendix, and displacing evaluate the upper scrotal sac,
Findings: superimposed gas-filled bowel loops. Patient cooperation maximizes the efficiency of the exam by spermatic cord and inguinal canals. Extratesticular and testicular vascularity should be evaluated
The intussusception presents as a mass with a hypoechoic rim and echogenic center or localizing the site of pain for the ultrasonographer. Visualization of the psoas and iliac vessels using color Doppler set to detect low flow velocities for the asymptomatic testis and then
multiple concentric rings of alternating echogenicity (the target sign). In the longitudinal plane indicate adequate penetration of the abdomen. compared. Power Doppler may be used but has higher sensitivity to low flow and is more
there are hypoechoic layers on each side of an echogenic center giving a pseudo-kidney susceptible to movement.
appearance or sandwich sign. Other findings can include free peritoneal fluid and trapped fluid Findings:
in the intussusception. Lead points can be found which include Meckel’s diverticulum, A normal appendix should be tubular, ≤ 6 mm in diameter, compressible and blind-ending. Findings:
duplication cysts and lymphoma (especially Burkitt lymphoma). An inflamed appendix is typically fluid-filled, non-compressible, and > 6mm in diameter. If transverse 1-3 hours: Normal testicular architecture. 4-6 hours: Enlargement and heterogeneous echogenicity
to the appendix, a target appearance is seen. An appendicolith is an echogenic focus with acoustic of the affected testis. The twisted spermatic cord (torsion knot) is seen as a redundant twisted
Tricks: shadowing. structure above the testicle. Presence of Doppler flow in the normal testis and absent or decreased
Look for the target sign. Trace the entire course of the intussusception. Look for signs of Tricks:
. flow in the affected testis. >24 hours: Heterogeneous echotexture, significant testicular
small bowel obstruction on ultrasound. Look for potential lead points. Try and distinguish Have the patient point to the region of maximal tenderness enlargement, marked hyperemia of the scrotal wall and paratesticular soft tissues and absent
ileocolic intussusception from small bowel-small bowel intussusception (size). and start there. Use color and power Doppler to localize testicular flow, all evidence of testicular infarction and necrosis (missed torsion).
the inflamed appendix. Coronal scanning along the flank
can find the occasional retrocecal appendix (Image 2). Tricks:
Use your other hand from behind to increase graded Image 2 Use transverse imaging of both testes to compare, including color Doppler flow. Set your color and
HYPERTROPHIC PYLORIC STENOSIS compression. spectral gains to the asymptomatic side and without changing settings, compare to the
symptomatic testis. Look for the torsion knot. Always scan the inguinal canal.
Technique:
A high frequency linear array OVARIAN TORSION
transducer is chosen Technique:
depending on infant size and A transabdominal approach is undertaken.
pylorus depth. The patient is Transvaginal imaging can be done if the patient is TORSION OF THE APPENDIX TESTIS
scanned in the supine position sexually active or has had a prior pelvic exam. The
Image 1 Technique:
and the probe in the transverse urinary bladder is filled by oral hydration, intravenous
plane immediately below the Same as for Testicular Torsion.
hydration or Foley catheter. Use of a curvilinear or a b
Xiphoid process. The gastric antrum is identified by sector transducer is typical. It should be remembered
air and fluid. If the stomach is distended with gas, that the ovary may be cephalad to the uterus or behind
repositioning the patient to left anterior oblique or right the bladder. Color Doppler is useful to compare ovarian
side down decubitus allows the antrum to fill with fluid blood flow, but its presence does not exclude ovarian
to better evaluate the pylorus. A useful technique is to torsion.
feed the infant Pedialyte or formula/breast milk before Findings: a b c d
repositioning the patient into right decubitus for clearer a Enlarged ovary, free fluid in the cul-de-sac and a
c d
visualization of the pylorus. If the stomach is b Fig 6. a. Homogeneous right testicle. b. Complex fluid collection surrounding the left testicle,
dilated fallopian tube. The most specific finding in Fig 4.follicles. b. Enlarged andin echotexture right
a. Left ovary normal with scrotal wall and skin thickening. c. Marked hyperemia within the left epididymis and left
distended, the pylorus is sometimes found by Fig 2: a. Enlarged pyloric muscle adolescents is a solid ovary with multiple, small 8-12 small with peripheral follicles and through-
heterogenous testicle. d. Heterogenous echogenic 9 mm x 5 mm left testicular appendage (arrow) without
scanning through the flank/liver. measuring 4 mm in thickness b. Pyloric ovary flow, consistent with torsion of the testicular appendix.
channel length of 14 mm. mm peripheral cysts - the “string of pearls” sign. Cysts transmission. c. and d. Flow along periphery of
Findings: and solid masses may be found in association and as right ovary anteriorly by color and spectral Doppler. Findings:
The pylorus is typically uniformly hypoechoic. The abnormal pyloric muscle should be ≥ 3-4 the cause of the ovarian torsion. Small hyperechoic or hypoechoic mass adjacent to superior aspect of testis or epididymal head.
mm and the pyloric channel ≥ 14-20 mm. Ancillary signs include the antral mucosal nipple Tricks: Associated finding include an enlarged and hypoechoic testicle and/or epididymis, reactive
sign- prolapsed pyloric channel mucosa into the gastric antrum, double-track sign- presence of Look for the “sting of pearls” sign. Look for uterine deviation towards the side of torsion. Have a high hydrocele and skin thickening. An infarcted appendix may calcify and detach, becoming a
linear sonolucent stripes of fluid in the crevices of the pyloric mucosa, minimal gastric index of suspicion when there is ovarian enlargement even with the presence of some Doppler flow. scrotolith. Color Doppler demonstrates epididymal/testicular hyperemia and the avascular torsed
emptying, appendix testis.
Tricks:
Use Pedialyte to outline the pylorus and move air to the fundus. Scan in left anterior oblique Tricks:
or right side down decubitus position. Use the liver as an acoustic window if the stomach is REFERENCES
Most prepubertal boys will have a torsed appendix testis as the cause of reactive “epididymo-
already overdistended. Scanning through the back can help in certain cases (Image 1) . 1. Aso C, Enríquez G, Fité M, et al. Gray-scale and color Doppler sonography of scrotal disorders in children: an update. RadioGraphics 2005; 25: 1197–1214. orchitis”, as compared to infection in older boys who are sexually active. Follow up ultrasound to
Identify the abnormal pylorus by its resemblance to the uterus (another thickened muscle). 2. Hernanz-Schulman M. Infantile Hypertrophic Pyloric Stenosis. Radiology 2003; 227:319-331. make sure this resolves is useful.
3. Puylaert JBCM. Acute Appendicitis: US Evaluation Using Graded Compression. Radiology 1986;158:355-360.
Avoid sector or curvilinear transducers. gastric dilatation with fluid and exaggerated peristaltic 4. Servas S, Zurakowski D, Laufer MR, et al. Sonographic findings of ovarian torsion in children. Pediatric Radiology 2007 May; 37 (5):446-451.
waves in the gastric antrum (pyloric teet). 5. Siegel MJ, ed. Pediatric sonography. 3rd ed. Philadelphia, Pa: Lippincott Williams & Wilkins, 2002.