
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Esophageal pH monitoring in pediatrics
Similar to Esophageal pH monitoring in pediatrics (20)
More from Samir Haffar
More from Samir Haffar (20)
Recently uploaded
Recently uploaded (20)
Esophageal pH monitoring in pediatrics
- 1. Esophageal pH monitoring in pediatrics Samir Haffar MD Assistant Professor of Gastroenterology
- 2. pH monitoring of the esophagus 24-hours pH monitoring Wireless pH monitoring pH-impedance monitoring (pH-MII)
- 3. 24-hours pH monitoring
- 4. 24-hours pH monitoring & medications • Antacid discontinued 6 hours before • Prokinetics discontinued 48 hours before • Anti-H2 receptor discontinued 3 days before • PPI discontinued 7 days before Do not use antacids/OTC medications during the study Fasting: 3 h for infants & 6 h for children over 1-year old
- 5. Location of pH electrode above LES 5 cm in adults and 3 cm in children
- 6. Why 3 cm above LES? • Has been standard for many years • Chosen to avoid catheter migration into stomach • Moving by a 1 cm or two would not change results • Moving it 10 cm above LES miss a number of patients who are identified by the more distal location
- 7. Location of LES • Manometric localization reference method • pH step-up method sudden rise to pH > 4 • Strobel’s formula* infants up to 1 year of age • LES locator porior to pH • Fluoroscopic techniques not accurate • Endoscopic technique not accurate * length from nostrils to LES in cm = [(height × 0.252) + 5] × 0.87 Wenzl TG et al. J Pediatr Gastroenterol Nutr 2012; 55: 230-234.
- 8. Acid reflux: pH ˂ 4 for ˃ 5 sec Why pH < 4? • Defined early in development of the technology • Marked difference from normal esophageal pH of 7 • Pepsinogen converted to pepsin at pH < 4 • pH < 4 is one that tends to produce symptoms • However, pH that do not reach level of 4.0 still represent reflux as demonstrated by pH-impedance
- 9. Device of 24-hours pH monitoring Using buttons provided on the device Diary: symptoms, body position (supine, standing) & eating
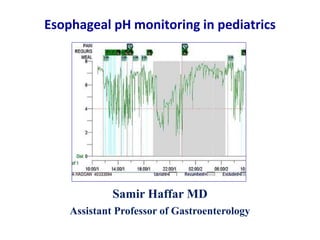
- 10. Normal 24-hours pH monitoring Quantitative analysis Qualitative analysis Bremner CG et al. Esophageal disease & testing. Taylor & Francis Group, 2005.
- 11. Quantitative analysis composite score Composite score calculated by the program Parameters Normal values % of total time pH <4 (acid exposure time) ˂10% (˂1 y),˂5% (˃1 y) % of upright time pH <4 % of supine time pH <4 No of reflux episodes <100 (<1 y), <70 (>1 y) No of reflux episodes >5 min < 8 episodes Longest reflux episode in min
- 12. Normal value of composite score • Boix-Ochoa < 11.99 • DeMeester < 14.72 • Johnson-DeMeester < 22 Boix-Ochoa score is the most accurate score to be used in pediatrics for GERD diagnosis Boix-Ochoa J et al. J Pediatr Surg 1980;15 (1): 74-78 DeMeester TR et al. Ann Surg 1976 ; 184 :459 – 470.
- 13. Comparison of DeMeester to Boix-Ochoa score • Sensibility 86% • Specificity 98% • Positive predictive value 99% • Negative predictive value 73% • Accuracy 90% • Pearson correlation coefficient r 0.9409 – p= 0.000 Lupu VV et al. Medicine 2016;95:26(e3804). Retrospective study of 234 children with suspected GERD
- 14. Qualitative analysis symptom-reflux correlation • Symptom index positive if ≥ 50% • Symptom sensitivity index positive if ≥ 10 % • Symptom association probability positive if ≥ 95% Determine relationship between symptoms & acid reflux events, regardless if pH test is normal or abnormal More reliable when at least 3 symptom events occur during test
- 15. Sites of 24-hours pH monitoring • Single site 3 cm above LES • Multiple sites 3 & 13 cm above LES 1 in esophagus & 1 in proximal stomach 1 in esophagus & 1 in hypopharynx
- 16. Distal & proximal esophageal pH monitoring
- 17. Nocturnal acid breakthrough Gastric pH <4 for at least 1 hour during the night in patients with persistent heartburn on standard dose PPIs twice daily Combined gastric & esophageal 24 hr pH monitoring
- 18. ‘off or on therapy’ monitoring • Off therapy (unproven GERD) No or low-grade esophagitis on endoscopy No prior positive pH testing Before anti-reflux surgery • On therapy (proven GERD) Double-dose PPI therapy & pH-impedance monitoring Correlation between refractory symptoms & reflux episodes Exclude inadequate acid suppression Exclude poor compliance
- 19. • SI, SSI & SAP cannot be compared with each other • SI & SAP are predictive of response to medical/surgical therapy Interpretation of 24-hours pH monitoring • % of total time pH <4 <10% (<1 year) – ˂5% (>1 year) predictive response to med/surg therapy • No of reflux episodes <100/24 h (<1 y) – <70/24 h (>1 y) Quantitative analysis (composite score) Qualitative analysis (symptom-reflux association) SI: symptom index – SSI: symptom sensibility index – SAP: symptom association probability Patra S et al. J Trop Pediatr 2011;57:99-103. Singendouk MMJ et al. Neurogastroenterol Motil 2016;28:1452–1459. Normal values available for several age groups but used with caution
- 20. Indications of esophageal pH monitoring • Diagnosis of acid related disorders: NERD, hypersensitive esophagus & functional heartburn Clarify role of acid in esophageal eosinophilia • Correlate persistent symptoms with acid GER events • Efficacy of acid suppression in high risk patients: Cystic fibrosis, neurologically compromised patients NASPGHAN: North American society of gastroenterology, hepatology & nutrition Rosen R et al. Pediatric GERD clinical practice guidelines. J Pediatr Gastroenterol Nutr 2018;66(3):516-554. Insufficient evidence to support routine use of pH monitoring for diagnosis of GERD in infants and children (NASPGHAN)
- 21. Wireless pH monitoring
- 22. Wireless pH monitoring Ayazi S et al. Clin Gastroenterol Hepatol 2009;7:60–7. Recording for a minimum of 48 hours Some studies reported recording up to 5 days
- 23. Rosen R et al. Pediatric GERD clinical practice guidelines. J Pediatr Gastroenterol Nutr 2018;66(3):516-554. Wireless pH monitoring Advantages Disadvantages increase diagnostic yield expensive useful in some patients: - developmental delay - autism - cystic fibrosis - chronic cough - exercise-induced GERD not widely available complications (0-15%): - esophageal tear - chest pain - failure to record - early detachment
- 25. Advantages of impedance • Content of bolus/refluxate liquid – gas – mixed • Direction of bolus anterograde – retrograde • Height of refluxate • pH characteristics acid reflux (pH-impedance) acid re-reflux weekly acid reflux weekly alkaline reflux
- 26. Liquid bolus high conductivity & low impedance Gastrointest Endoscopy Clin N Am 2005 ; 15 : 257 – 264. Single measuring site Drop in impedance to less than 50% of baseline values
- 27. Air belch/air swallow low conductivity & high impedance Single measuring site Rapid and pronounced rise in impedance (>3000 ohms) ohm: unit of measure for impedance Gastrointest Endoscopy Clin N Am 2005 ; 15 : 257 – 264.
- 28. Mixed air-liquid bolus Gastrointest Endoscopy Clin N Am 2005 ; 15 : 257 – 264. Single measuring site
- 29. Liquid swallow in impedance antegrade bolus movement Progression of impedance from proximal to distal ohm: unit of measure for impedance Gastrointest Endoscopy Clin N Am 2005 ; 15 : 257 – 264.
- 30. Liquid reflux in impedance retrograde bolus movement Progression of impedance from distal to proximal ohm: unit of measure for impedance Gastrointest Endoscopy Clin N Am 2005 ; 15 : 257 – 264.
- 31. Combined pH-impedance probe age-appropriate probes Bremner CG et al. Esophageal disease & testing. Taylor & Francis Group, NY, 1st edition, 2005. • pH orifice 5 cm from the tip • Impedance orifices 3, 5, 7, 9, 15, & 17 cm from the tip • MII-pH probe = pH probe Do not change patient comfort
- 32. GERD classification by pH-impedance monitoring Acid reflux Reflux with drop of pH from above 4.0 to below 4.0 Superimposed acid reflux (acid re-reflux) Acid reflux occurs while pH < 4.0 Weakly acidic reflux Reflux results in esophageal pH between 4.0 & 7.0 Weakly alkaline reflux Reflux with nadir esophageal pH does not drop <7.0 Sifrim D et al. Gut 2004 ; 53 ; 1024 – 1031.
- 33. Weakly acid reflux in pH-impedance monitoring Sifrim D et al. Best Pract Research Clin Gastroenterol 2009;23:369–386.
- 34. pH-impedance monitoring Advantages Disadvantages Acid re-reflux not widely available Weakly acid reflex (pH 4.0 – 7.0) higher cost* Weakly alkaline reflux (pH ˃7.0) limited reference value** Liquid & gas reflux Higher sensitivity compared to pH-metry * Cost of pH-impedance probe: 150 € ** Pilic D et al. German Pediatric Impedance Group. J Pediatr 2011;158:650–4.e1.
- 35. Indications of pH-impedance monitoring • Differentiate NERD, hypersensitive esophagus & functional heartburn in patients with normal endoscopy • Clarify role of acid & non-acid reflux in etiology of esophagitis and other signs and symptoms suggestive for GERD • Correlate troublesome symptoms w acid & non-acid GER events • Determine the efficacy of acid suppression therapy Rosen R et al. Pediatric GERD clinical practice guidelines. J Pediatr Gastroenterol Nutr 2018;66(3):516-554. Insufficient evidence to support use of pH-MII as single technique for diagnosis of GERD in infants and children (NASPGHAN)
- 36. Erosive Esophagitis 30 % Endoscopy-Negative Reflux Disease (ENRD) Up to 70 % GERD Functional Heartburn 50 % Normal acid exposure Normal SI & SAP SI: symptom index – SAP: symptom association probability Giacchino M et al. Ann Gastroenterol 2013;26:283-9. Non-Erosive Reflux Disease (NERD) Hypersensitive esophagus Normal acid exposure Abnormal SI & SAP to acid/non-acid reflux
- 37. Clinical observation • 8-year-old boy w/o prior disease complained of heartburn • PPI not effective • UGI endoscopy WNL • Esophageal biopsies Absence of EE • Esophageal manometry WNL • 24-hours pH-impedance Acid exposure time 4%/24 hours SI for acid reflux normal (35%) SAP for acid reflux normal (75%) What is the diagnosis? EE: eosinophilic esophagitis – SI: symptom index – SAP: symptom association probability – WNL: within normal limit
- 38. Clinical observation • 8-year-old boy w/o prior disease complained of heartburn • PPI was not effective • UGI endoscopy WNL • Esophageal biopsies Absence of EE • Esophageal manometry WNL • 24-hours pH monitoring Acid exposure time 4%/24 hours SI for acid reflux normal (35%) SAP for acid reflux normal (75%) What is the diagnosis? Functional heartburn What is the treatment? EE: eosinophilic esophagitis – SI: symptom index – SAP: symptom association probability – WNL: within normal limit
- 39. Clinical observation • 8-year old boy w/o prior disease complained of heartburn • PPI was not effective • UGI endoscopy WNL • Esophageal biopsies Absence of EE • Esophageal manometry WNL • 24-hours pH monitoring Acid exposure time 4%/24 hours SI for acid reflux normal (35%) SAP for acid reflux normal (75%) What is the diagnosis? Functional heartburn What is the treatment? Trazodone or SSRI EE: eosinophilic esophagitis – SI: symptom index – SAP: symptom association probability – WNL: within normal limit
- 40. Thank You
- 41. Symptom Index (SI) positive if ≥ 50 % Not take into account overall number of reflux episodes Number of reflux-related symptom episodes Total number of symptom episodes x 100
- 42. Symptom Sensitivity Index (SSI) positive if 10 % Not take into account overall number of symptoms Number of symptom-related reflux episodes Total number of episodes x 100
- 43. • Also known as Binomial Symptom Index (BSI) • More complex statistical calculations Divide tracing into 2-min segments & looks at whether a symptom & acid are present during each 2 min segment • Take into account all relevant components: Reflux episodes Total numbers of symptom events Reflux-related symptom events Symptom Association Probability (SAP) positive if ≥ 95% Gyawali CP et al. Gut 2018;67(7):1351-1362.
- 44. Number of reflux episodes/24 hours in children Available reference values Singendouk MMJ et al. Neurogastroenterol Motil 2016;28:1452–1459.
Editor's Notes
- Intragastric pH Monitoring: The evidence supporting the clinical significance and applicability of gastric pH monitoring is insufficient to recommend its routine use in clinical practice. Proximal pH Recording: available evidence does not support the routine use of proximal pH monitoring in clinical practice.
- Relatively new technique developed in early 1990s at Helmholtz Institute in Aachen (Germany) Silny* provided first description of this technique that assesses intraluminal bolus movement by measuring changes in conductivity of intraluminal content
- High failure rate (25%) of the wireless pH capsule - premature detachment - dropped signals - severe side effects
- Relatively new technique developed in early 1990s at Helmholtz Institute in Aachen (Germany) Silny* provided first description of this technique that assesses intraluminal bolus movement by measuring changes in conductivity of intraluminal content