Mrcp 2 dermatology
•
110 likes•13,937 views

MRCP contact me at (sherif_badrawy@yahoo.com)

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Mrcp 2 dermatology
Similar to Mrcp 2 dermatology (20)
More from Sherif Elbadrawy
More from Sherif Elbadrawy (16)
Recently uploaded
Recently uploaded (20)
Mrcp 2 dermatology
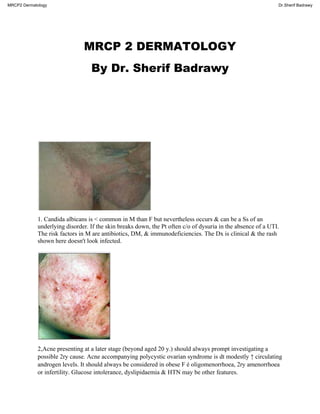
- 1. MRCP 2 DERMATOLOGY By Dr. Sherif Badrawy 1. Candida albicans is < common in M than F but nevertheless occurs & can be a Ss of an underlying disorder. If the skin breaks down, the Pt often c/o of dysuria in the absence of a UTI. The risk factors in M are antibiotics, DM, & immunodeficiencies. The Dx is clinical & the rash shown here doesn't look infected. 2,Acne presenting at a later stage (beyond aged 20 y.) should always prompt investigating a possible 2ry cause. Acne accompanying polycystic ovarian syndrome is dt modestly ↑ circulating androgen levels. It should always be considered in obese F é oligomenorrhoea, 2ry amenorrhoea or infertility. Glucose intolerance, dyslipidaemia & HTN may be other features. MRCP2 Dermatology Dr.Sherif Badrawy
- 2. 3.Dermatomyositis is an AI skin condition ➜ insidious, symmetrical, proximal ms weakness dt ms inflammation. AutoAbs to striatal ms are found . The skin Ss are characteristic: • heliotrope rash: lilac discolouration around eyes • malar erythema & facial oedema • Gottren's papules (seen in picture): lilac atrophic papules over knuckles • erythema & telangiectasia of nail folds . The skin Ss can appear much earlier than the ms symptoms. Malignancy is assoc. é dermatomyositis in up to 30% of Pts > the age of 40 y.. The neoplasias MC seen are breast, lung, ovary & stomach. In this gentleman it probably coincides é a stomach malignancy. Rx is é ↑dose steroids & immunosuppressants. Rx of the driving malignancy often leads to resolution of the cutaneous symptoms. MRCP2 Dermatology Dr.Sherif Badrawy
- 3. 4.This gentleman has HHT which is an AD condition. Small red macules & papules on the lips, tongue & fingers, assoc. é nose bleeds & GI bleeding. Anaemia dt bleeding is Rx é oral iron. The skin lesions do not need any Rx although pulse dye laser is very effective at removing them if unsightly. Peutz.Jegher's syndrome is another rare genetically determined condition which ➜ brown macules on the lips, the skin around the mouth & the fingers & toes, occurring early in childhood. It Is assoc. é small bowel polyps which can cause intussusception. 5.Erythema multiforme involving the mouth presents é multiple irregular erosions on the buccal mucosa. Extensive involvement of the mouth, lips, conjunctiva & genitalia is called Stevens-J MRCP2 Dermatology Dr.Sherif Badrawy
- 4. ohnson syndrome. The causes of this are similar to of erythema mutiforme but are > likely to be drugs e .g. co-trimoxazole. 6.This lesion is dt needle marks from IV injection. She ➜ Rx é naloxone to reverse the opiate overdose. Non-fatal overdose is common among heroin injectors · one study found overdose in 2/3 of people abusing iv heroin. Overdose is also strongly dt polydrug use, é the risk of this ↑ in relation to other drugs of abuse being taken (methadone, temazepam, alcohol etc). mortality ratio. 7.Alopecia areata (AA) is a condition ➜ recurrent non-scarring patches of hair loss can affect any hair-bearing area of skin. In the areas affected, the skin is normal in appearance but ± short, broken hairs taper at the proximal end (exclamation point hairs) - this is a pathognomonic Ss but is not always present. Pts may also c/o of pruritus or a burning in the affected skin areas. A +ve pull test at the periphery of an affected area indicates the dis. is active & further hair loss may occur. AA can occur at any age & affects both sexes equally. The natural Hx of the condition is unpredictable é no correlation existing bw the number of patches at onset & the subsequent severity of the dis.. Ppt factors, ex. a major life event, a febrile illness, drugs & pregnancy, can be found in some Pts é AA but most Pts fail to report a triggering factor preceding their episode of hair loss. Ringworm is a superficial fungal infection of the skin begins as a small erythematous papule which spreads forming numerous papules in a typical ring form. The Pt may c/o of intense pruritus. Although AA may be assoc. é atopic dermatitis (AD), a chronic pruritic condition usu. begins in infancy é characteristic skin changes. MRCP2 Dermatology Dr.Sherif Badrawy
- 5. 8.There are 3 categories used to describe HPV infections based on their clinical Ss: anogenital and/or mucosal, nongenital cutaneous & epidermodysplasia verruciformi.The cutaneous variety usu. produces benign, selflimiting warts which are usu. found on the hands & fingers. The term 'kissing warts' has been applied to this kind of infection dt the autoinoculation may occur from a wart on one finger ➜ the occurrence of warts on an adjacent finger. The virus can be spread by direct or indirect contact & can resist desiccation, freezing & prolonged storage outside of host cells. The Dx is made primarily on the clinical findings. MRCP2 Dermatology Dr.Sherif Badrawy
- 6. 9.The story is typical of scabies. Scabies is generally MC in children & young adults, in recent y. the incidence has been ↑ in the elderly in nursing & residential homes. Itch is the MC manifestation of scabies & occurs at night when the Pt is warm. The pathgnomic lesions of scabies are burrows, people also develop a hypersensitivity reaction in the form of papules. lichen planus can also be itchy & affect the wrists but is usu. purple in colour é white striae. 10.Humans are unable to synthesise ascorbic acid, & vitamin C deficiency ➜a condition known as scurvy. The initial typical skin changes are of follicular keratosis é coiling of hair. later, Pts develop perifollicular hge, bleeding gums & purpura over the legs. Pts often have an assoc. anaemia & their plasma ascorbic acid levels will be ↓. There is a rapid response to Rx. MRCP2 Dermatology Dr.Sherif Badrawy
- 7. 11.Photosensitivity is MC é amiodarone. Frusemide & thiazide but < usu. so. Allopurinol may cause a vasculitic rash & over-anticoagulation é warfarin may lead to purpura & haematomas é minimal trauma. 12.This mother & son have scabies - red/brown papules & nodules on the penis & scrotum are pathognomonic for this condition. The whole household ➜ Rx & linen etc washed at 60 ·c. Rx may worsen the itch for a few days & itching may persist for up to 2 weeks post effective Rx - antihistamines & calamine lotion may help. 13.This is Reiter's syndrome & the rash is keratoderma blenorrhagica. It occurs 2ry to Chlamydia trachomatis (which may also cause circinate balanitis as in this case), salmonella, shigella, Campylobacter jejuni & yersinia. Stool ➜ cultured if diarrhoea is present & a urethral swab/sexual review, as urethritis may be asymptomatic. The arthritis is Rx by rest, NSAIDs ± steroids & does not tend to respond to Rx of the causative organism. 14.This lady's rash is erythema ab igne, which is dt long-term heat exposure (often sitting close to electricfgas fires or from hot water bottle application for chronic pain relief). This Pt therefore must feel the cold & + a suggestion of myxoedematous facies, the Dx is hypothyroidism. Livedo reticularis is also a reticular rash, often affecting LL, & this may be physiological, assoc. é antiphospholipid Ab syndrome, SLE or other CT dis.. Cushing's dis.fsyndrome causes striae. MRCP2 Dermatology Dr.Sherif Badrawy
- 8. 15.This describes scurvy, vitamin C (ascorbic acid) deficiency, which ➜reduction in collagen formation & assoc. capillary fragility. It occurs in people é poor dietary intake, who eat little or no fruit & vegetables, commonly alcoholics & elderly people existing on a 'tea & toast' diet. Pregnancy, lactation & thyrotoxicosis ↑ ascorbic acid requirements & may ppt scurvy. The normo normo anaemia reflects bleeding into tissues, normal platelet count excludes thrombocytopenia. Zinc deficiency ➜well-demarcated psoriasiform & eczematous-like plaques, initially occurring in perioral & anogenital areas. 16.These nails grow slowly & are thickened, curved & yellow- this suggests yellow nail syndrome, which is usu. assoc. é lymphatic hypoplasia (check for lymphoedema of extremities). The syndrome can be assoc. é a number of pulmonary conditions including bronchiectasis, pleural effusion COPD or neoplasm. It is also assoc. é nephrotic syndrome & penicillamine use. 17.Dermatitis herpetiformis (DH) is an AI blistering disorder assoc. é a gluten-sensitive enteropathy. It ➜ gped excoriations; erythematous, urticarial plaques; & papules é vesicles. These are located on the extensor surfaces of the elbows, knees, buttocks, & back. extremely itchy & vesicles are often excoriated to erosions. Dx by direct immunofluorescence of a skin biopsy specimen showing deposition of Ig A in a granular pattern in the upper papillary dermis.It is Rx é dapsone & é maintenance of a gluten-free diet. Coeliac dis. is a chronic AI disorder of the MRCP2 Dermatology Dr.Sherif Badrawy
- 9. small intestine dt gluten intolerance in genetically predisposed individuals. It ➜ mucosal lesions of the small bowel ➜malabsorption. < 10% of Pts é DH exhibit Sx of an underlying gluten- sensitive enteropathy. > 90% of Pts show abnormalities upon endoscopic examination. 18.erythema nodosum, which may affect parts of the body other than the shins. She is from Morocco & so TB is ↑ on the DD. The only other physical finding is the tenderness on vaginal examination & this pathology in the ovarian tubes suggests a Dx of U/L salpingitis 2ry to TB. This can occur in the absence of respiratory infection or signs. MRCP2 Dermatology Dr.Sherif Badrawy
- 10. 19.Lichen planus is of unknown aetiology. Its association é AI dis. like vitiligo, alopecia areata & ulceratlve colitis suggests it too can be mediated immunologically. Typical lesions are violaceous or lilac-coloured intensely itchy flat topped papules arising on the extremities. Genital skin is similarly affected in the absence of oral, nail or other skin findings. In 50% of Pts there are oral lesions e.g. white asymptomatic lacy lines, dots or plaques. In 10% of Pts there are nail changes e.g. longitudinal ridging & destruction of the nail bed. Potent topical steroids are the DOCH. 20.Impetigo is a common superficial infection of the epidermis occurring mainly in children. It is usu. dt Staphylococcus aureus, a gp A beta-haemolytic streptococcus or a mixture of both. organisms gain entrance through broken skin (cuts & grazes) It is very contagious. typically starts as vesicles which then break down to form honey-coloured crusts. 2 forms of the condition, bullous & non-bullous, é the former being caused almost exclusively by Staphylococcus aureus but the latter can be dt S. aureus, gp A streptococcus (Streptococcus pyogenes), or a combination of both. The non-bullous form tends to affect children but the bullous form can affect all ages. Because the infection is very superficial, topical antibiotics are > effective than systemic. Once thick crust is removed, topical antibiotics ex. 2% mupirocin (Bactroban), 2% fusidic acid (Fucidin) or 0.3% neomycin ointment ➜ used. It should also be applied to the Ant. nares at the MRCP2 Dermatology Dr.Sherif Badrawy
- 11. same time. Oral penicillin V is useful in parts of the world where impetigo is dt a gp A beta- streptococcus, to prevent acute GN occurring. Herpes simplex infection dt HSV type I is often recurrent & always recurs at the site at which the 1ry infection was e.g. the mouth. Most Pts experience a prodromal sensation of itching, burning or tingling. A few h later small gped vesicles appear, burst, crust & then heal in 7-10 days. These episodes can be ppt by fever, hence the name 'cold sore' . Herpes simplex can be DD from impetigo by the Hx of recurrent episodes, prodromal pain & initial vesicles containing clear fluid . In adults it is > likely than impetigo. If in doubt viral PCR will confirm the Dx. 21. rhinophyma - localised swelling of soft tissue é variable combinations of sebaceous hyperplasia, fibrosis & lymphoedema. Sebaceous hyperplasia is a recognised SE of ciclosporin Rx, esp. on the skin of renal transplant Pts when exposed to sunlight. Rosacea is a rash which although > common in F occurs in M & is assoc. é rhinophyma. It is an erythema of the face é telangiectasia. It is similar to acne in there are papules & pustules but no comedones. Complications ex. blepharitis, chronic lymphoedema of the face & rhinophyma occur > commonly in men. Rx of the rhinophyma by surgical excision or physical ablation of excess tissue may improve cosmetic appearance. MRCP2 Dermatology Dr.Sherif Badrawy
- 12. 22.Steroid rosacea is dt topical steroids to the face usu.. a large number of people use other family members' creams & ointments without seeking advice from the doctor 1st. It is important to ensure you question the Pt about use of all topical Rxs. Contrary to popular belief, it is not assoc. é excessive alcohol intake. Skin cancers, despite being > common in renal transplant Pts always present as ulcerative nodular Lesions before infiltrating deeper. Active rosacea ➜ Rx é oral antibiotics in the 1st instance. 22.This lady has a common condition found on elderly care wards · retention hyperkeratosis. The Rx for varicose eczema in the past é bandages were changed inusu. interferes é the normal process of Desquamation & results in this condition - a build up of keratin. It is a benign but malodorous condition can be Rx very well é gentle debridement after soaking in arachis oil, revealing normal skin underneath. Recurrence can be prevented by skin care é emollients. 23.The causes of Stevens-Johnson syndrome are the same as for erythema multiforme but usu. drugs are the cause rather than infections. It is therefore imperative to stop all drugs in the 1st instance. There is no evidence systemic steroids are helpful. Iv Igs are useful in the Rx of TEN. MRCP2 Dermatology Dr.Sherif Badrawy
- 13. Antibiotics are not useful. Throat swab for streptococcus & chest X-ray looking for mycoplasma pneumoniae are useful steps in the Rx but not the initial steps. 24. Herpes zoster occurs in people who have previously had chickenpox. The virus Herpes varicella-zoster lies dormant in the dorsal root ganglion after chicken pox, & later travels down the cutaneous nerves to infect the epidermal cells. The prodromal period is fol↓ed by a rash consisting of a gp of vesicles on an erythematous background, fol↓ed by weeping & crusting; healing takes 3-4 weeks. The rash is nearly always U/L & confined to one or 2 dermatomes. Oral antiviral agents ex. aciclovir at a ↑ dose are only beneficial if given in the 1st 48 h of the development of blisters. Regular analgesics are important, but in the elderly esp. if given as soon as the rash appears, prophylactic amitriptyline at night starting at 25 mg & ↑ to 75 mg can help prevent post-herpetic neuralgia. Topical aciclovir is of no benefit at all. 25.A malignant melanoma is a malignant tumour of the melanocytes. 2/3 a↑ from normal skin & 1/3 a↑ from a pre-existing mole. Superficial spreading malignant melanomas occur as malignant melanocytes migrate laterally along the derma-epidermal junction, & have a good prognosis. It is MRCP2 Dermatology Dr.Sherif Badrawy
- 14. important to diagnose melanomas while they are thin so removal ➜cure. Pigmented BCCs are heavily pigmented lesions but have the appearance of a BCC -nodules é rolling edges. 26.This lady has tinea corporis. This is dt dermatophyte fungi of the Microsporum, Trichophyton & Epidermophyton species. It presents é an asymmetrical erythema & itching é a well· defined edge. It is very important to obtain mycological confirmation of the Dx from skin scrapings before starting Rx. Since the infection of dermatophytes is in the keratin layer on the surface of the skin, topical Rx works better than systemic Rx. Fungicidal drugs ex. terbinafine or imidazoles (e.g. itraconazole) are effective. 27.Most women who c/o of flushing do suspect the menopause, but it is important to remember the other causes. Pts c/o of assoc. Sx of sweating waking them at night are likely to be menopausal. Sx of anxiety and hyperthyroidism (another common cause of flushing) can often be confused. CCBs are a common cause of facial flushing, which can often be continuous & persistent. MRCP2 Dermatology Dr.Sherif Badrawy
- 15. 28. scabies is most likely has an ill-defined eczematous rash which is not entirely typical of any other condition. Scabies is an infestation with the human scabies mite Sarcoptes scabei. transmitted by prolonged skin-to-skin contact é someone who had it. A fertilised F has to be transferred for the infestation to take place. She will then find a place to lay her eggs (a burrow); 4-6 weeks later a 2ry hypersensitivity rash occurs. This ➜ intense itching esp. at night. The Dx is confirmed by finding one or > 'burrows' in the finger web spaces. These are linear S-shaped papules 3-5 mm in length along the sides of the fingers or the front of the wrists. Rx is é D. 5% malathion lotion. It is necessary to Rx all those in close contact even if asymptomatic, which means the entire residential home ➜ Rx in the same way. 29.This gentleman has pityriasis versicolor - a scaly rash of varying colours. In different skin types it may be white, orange-brown or dark brown. The lesions are small, < than 1 cm in diameter, usu. round & always scaly when scratched. It is a dis. of young adults & occurs predominantly on the upper trunk. It is dt an infection é a yeast, Pityrosporum orbicular&, which we all have on our skin as a harmless commensal. Under certain conditions, the yeast produces hyphae & becomes pathogenic when it is known as Malassezia globosa. The depigmentation in darker skin types is dt suppression of melanin production by the pityrosporum yeast. 30.Oral hairy leucoplakia (OHL) is an oral mucosal dis. assoc. é EBV & occurs almost exclusively in Pts who are immunocompromised, esp. those infected é HlV. + being a Ss of AIDS, it is described + IBD & Behcet's. It is non-painful & the appearance of the white plaque may change slightly from day to day. Smoking > a pack of cigarettes a day is correlated +vely é development of OHL in men who are HlV +ve. The risk of developing OHL doubles é each 300-unit ↓in CD4 MRCP2 Dermatology Dr.Sherif Badrawy
- 16. count. Dx is clinical, though biopsy may be helpful in some cases to exclude dysplasia or malignancy. Rx is of the underlying disorder, most often é anti-retroviral Rx. 31.Seborrhoeic keratoses very common harmless skin growths 1st appear during adult life- commonest benign tumour in older individuals. also be called basal cell papillomas, senile warts or brown warts. They can itch, grow, & become cosmetically unattractive. Scratching seborrhoeic keratoses or trying to pick them off the skin can ➜a 2ry infection sometimes they’re many & they may obscure the detection of a dysplastic nevus or malignant melanoma. SCC or BCC can rarely develop + a seborrhoeic keratosis. 32.Discoid lupus erythematosis This is a chronic, scarring, photosensitive dermatosis. A small number of Pts with DLE may later develop SLE & DLE can occur as a feature of SLE. DLE usu. occurs as a skin manifestation alone without significant systemic features; some cases will have +ve autoAbs (Rh factor) + ↓ complement levels. Arthralgia may occur, & pruritis at the site of the lesions, but Pts are often asymptomatic. DLE may be localised (head & neck) or widespread as in this case. Rx is é sun protection, topical CST, oral antimalarial agents, & in severe cases systemic immunosuppressive Rx. MRCP2 Dermatology Dr.Sherif Badrawy
- 17. 33. Recurrent painful oral aphthous ulcers are the MC lesions assoc. with Behcet’s dis. & occur in 99.3%. Genital ulcers may also be present. 50% of Pts who have Behcet’s dis. develop GI symptoms: intestinal erosions & ulcers may cause abdominal pain, melena, & perforation. This may simulate Crohn' s dis. & other IBDs. Ocular involvement is seen in about 70% of Pts who have Behcet's dis.; most often Ant. or posterior uveitis. ocular Sx fol↓ the oral & genital ulcers by 3-4 y.,musculoskeletal; skin (erythema nodosum, acneiform lesions, thrombophlebitis, & cutaneous hypersensitivity); central & peripheral nervous system ,vascular lesions (thrombosis, aneurysm formation) . The cause & pathogenesis of Behcet’s dis. remain unknown, but the TNF- alpha is involved in the pathophysiology. Biopsies ➜vasculitis near lesions of Behcet's syndrome, including the oral & genital ulcers & lesions of the CNS & in the eyes; large vessels are affected by a vasculitis of the vasa vasorum. 34. dermatitis herpetiformis (DH), an immune-mediated blistering skin dis. é an assoc., most often asymptomatic, gluten-sensitive enteropathy. The rash is characteristically very itchy é blistering lesions over extensor surfaces. Although all Pts é DH by definition have gluten- sensitive enteropathy, < 10% of Pts have bloating, diarrhoea, or symptomatic malabsorption. deposition of IgA at the dermal-epidermal junction of the skin. IgA-circulating immune complexes are present in Pts é DH, although no association é dis. severity. These immune complexes also have been noted in Pts é isolated GSE, & believed to be dt the presence of the gut dis.. Assoc. of DH include GI & AI dis.. Coeliac dis. (gluten sensitivity in absence of DH) usu. involves > severe & widespread intestinal involvement. An ↑ risk is seen of GI lymphomas & non-Hodgkin 's lymphoma. 1st-line Rx is é dapsone➜rapid improvement. Gluten-free diet may also improve or control the Sx (al↓ ing D/C of dapsone), but requires a very motivated Pt, as the diet may be unpalatable. Dapsone is usu. Given initially because it al↓ s for faster recovery compared to gluten free diet a lone. 35. multiple cutaneous neurofibromata é a few cafe-au-lait spots. Criteria for Dx are: • six or > cafe-au-lait spots • 2 or > neurofibromas • axillary freckling • 2 or > Lisch nodules (iris hamartoma) MRCP2 Dermatology Dr.Sherif Badrawy
- 18. • optic glioma • a parent or sibling é neurofibromatosis assoc. abnormalities are: • skeletal rib notching & other bony defects • honeycomb lung • intellectual disability • kyphoscoliosis • HTN (renal artery stenosis, phaeochromocytoma) • Lisch nodules (iris hamartoma). 36. erythema multiforme. classical target lesions. 3 zones: a central area of dusky erythema, a middle paler zone of oedema & an outer erythematous ring. The lesions preferentially involve the extremities & trunk. They usu. appear in successive crops & fade in 1 to 2 weeks. There are multiple triggering factors although the cause is not determined in up to 50% of cases. MC association is é preceding herpes simplex or mycoplasma infection, although drugs ex. sulphonamides & penicillins are also usu. implicated.Orf is a < common aetiological trigger seen in farmers exposed to the virus. 37. erythema nodosum ➜ painful erythematosus nodules, appear on the Ant. aspect of the leg. The rash appears MC in young women & can either be idiopathic or 2ry to various disorders or drugs. The MC cause is infection, typically gp A beta haemolytic Streptococcus, therefore an ASO titre ➜ requested. Although < common, sarcoid & TB should not be missed ➜ a chest X- ray is essential. Other causes Rx ex. sulphonamides, pregnancy & IBD. Pt with no other Sx a colonoscopy would not be warranted. MRCP2 Dermatology Dr.Sherif Badrawy
- 19. 38. The Dx is Lyme dis.. dt infection by Borrelia burgdorferi transmitted to humans by tick bites. This Dx rash is erythema chronicum migrans. appears at the site of the tick bite in about 90% of Pts, around 9 days after the inoculation.enlarging ring formation, which may clear in the centre leaving a target-like morphology. Dissemination may ➜arthritis, neural involvement & heart dis., esp. conduction defects. Most non-disseminated dis. responds well to oral antibiotics eg doxycycline or arnoxicillin. 39. pemphigus. The blisters are flaccid as compared with pemphigoid, which presents é tense blisters & immunofluorescence along the BM. Most Pts also have mucosal lesions. The severity & Hx are variable but before Rx é steroids most Pts would die. Pts require ↑Dose steroids to induce remission & then may require long-term ↓er dose steroids for maintenance, usu. for around 2 y.. 40.Multiple neurofibromas are part of neurofibromatosis type 1 or von Recklinghausen 's dis.. It ➜ six or > cafe au lait spots, axillary freckling & Lisch nodules (pigmented iris hamartomas). The inheritance is AD & the gene is located on chromosome 17. Neurological cp seen in around 40% of Pts, MC an optic nerve glioma. Neurofibromatosis type 2 {NF2) ➜ B/L acoustic neuromas & other CNS tumours. Cafe au lait spots & cutaneous neurofibromas are much < common in NF2 & are usu. fewer in number. Periungual fibromas are part of the characteristic lesions for tuberous sclerosis. MRCP2 Dermatology Dr.Sherif Badrawy
- 20. 41.A heliotrope rash around the eyes & violaceous papules (Gottron 's papules) over the hands is characteristic of dermatomyositis. polymyositis, affects the proximal ms, eg brushing hair, standing up from a chair. 2 peaks of onset, one in childhood & the other bw the ages of 40 & 60 y.. Dermatomyositis occurs twice as usu. in women dt does in men. association é malignancy, commonly of the lung, breast, F genital tract, stomach & rectum. Dermatomyositis precedes the neoplasm in 40% of cases, both conditions occur together in 26%, & in 30% the neoplasm occurs 1st. Anti-Jo are the MC circulating Abs & are seen > commonly in Pts with pulmonary fibrosis. A DD is sarcoid, does not have the same predilection for eyes & hands but is assoc. é a ↑ serum ACE. 42.PCT is the MC of the porphyries.fragility & blistering of exposed skin. PCT is dt deficiency of uroporphyrinogen decarboxylase. scarring alopecia after resolution of bullae on the scalp, hypertrichosis & hyperpigmentation. Risk factors include alcohol & sun, both of which this lady ± been exposed to in Cyprus. AIP is not assoc. é cutaneous Ss. SLE is usu. photosensitive but does not present é blistering. Pompholyx is an intensely itchy form of eczema, over the hands & may present é multiple small blisters. 43.Acanthosis nigrans is a diffuse velvety thickening & hyperpigmentation of the skin. mainly in the axillae & other body folds. linked é various endocrine disorders (insulin resistance ex. DM, acromegaly & Cushing's syndrome, hypo- not hyperthyroidism). also occur as a complication of obesity. > rarely it is a paraneoplastic manifestation esp. of the GIT. MRCP2 Dermatology Dr.Sherif Badrawy
- 21. 44. This boy has a purpuric rash over his legs & buttocks, most likely to be HSP. reinforced by abdominal pain, which is a common association. GI bleeding is present in 50-75% of Pts. Renal involvement is also common although usu. mild with only haematuria or minimal proteinuria. Arthritis is also common affecting 75% of Pts. Perivascular IgAdeposits are characteristic & help to DD HSP from other vasculitic disorders. Mouth ulcers are not assoc. with this condition. 45.Necrobiosis lipoidica (NL) is > often in people é DM, in people é a FH of DM or a tendency to get DM. the exact cause of NL in not known.future DM development when it occurs in non- diabetic subjects. Most NL occur in the pretibial area, but cases have present on the face, scalp, trunk, & upper extremities, where the Dx is > likely to be missed. difficult to Rx although topical & intralesional steroids have been used. Inhibition of platelet aggregation é aspirin may be helpful. Granuloma annulare is a benign inflammatory dermatosis characterised clinically by dermal papules & annular plaques. Pyoderma gangrenosum ➜ violaceous nodules & plaques, many é central crusting & ulceration é undermisned borders. Plaque sarcoidosis ➜ round-to oval, red-brown to purple infiltrated plaques; the centre of the plaque may be atrophic. Acanthosis nigricans ➜ symmetric velvety hyperpigmented plaques é thickened skin. 46. alopecia areata (AA) a condition of unknown aetiology assoc. é other AI dis., ex. Hashimoto's MRCP2 Dermatology Dr.Sherif Badrawy
- 22. thyroiditis (hence the importance of checking the TFTs), vitiligo & MG. no curative Rx available although systemic steroids induce remission, AA recurs on D/C & the risk of long-term Rx precludes its use. a very distressing, & although it often spontaneously remits, psychological support from family, doctor & support gps is important. DD includes white-patch tinea capitis (for which anti-fungals are appropriate). Topical minoxidil may be helpful in M pattern baldness. 47. psoriasis - extensor skin on knees is affected by a purplish plaque é silvery scales. Troublesome psoriasis or assoc. severe arthritis justifies use of DMARDS ex. methotrexate. LFTs & FBC must be monitored regularly- SEs hepatitis & liver cirrhosis, lung fibrosis. Cyclosporin causes nephrotoxicity & U+Es & creatinine must be checked regularly + BP (may ppt HTN). Calcipotriol ointment is used for bd topical Rx of plaque psoriasis. 48. Pyoderma gangrenosum occurs when an inflamed nodule or pustule breaks down centrally to form an expanding ulcer é a characteristic undermisned bluish edge.usu. occur over the site of surgery - demonstrating pathergy.commonly occurs at sites of trauma. pathogenesis (probably immunological) is not fully understood. It can occur without underlying dis. but tends to be assoc. with: • ulcerative colitis • conditions ➜ polyarthritis e.g. RA • Crohn's dis. • monoclonal gammopathies • leukaemia (bullous form of pyoderma) can be single or multiple. Rx is é ↑ dose steroids ± cyclosporin. but not antibiotics, & they usu. heal leaving papery scars. MRCP2 Dermatology Dr.Sherif Badrawy
- 23. 49. pigmented macules (lentigines) on the lips, around the mouth & buccal mucosa (not on the tongue), palm & soles assoc. é intestinal polyposis (hamartomas which may occur in small & large bowel) describes the Peutz-Jeghers' syndrome. Malignant transformation of these polyps is rare but it is assoc. é ↑ risk of breast, ovarian & pancreatic cancer. Co-existent gastric adenomas may occur, ➜ an ↑ risk of gastric cancer. Pts may present é complications ex. iron deficiency anaemia, frank Gl hge, intestinal obstruction or intussusception, recurrent abdominal pain. Addison's dis. (which would cause hyponatraemia) ➜a > generalised hyperpigmentation, esp. buccal mucosa & palmar creases. 50.sarcoidosis é the picture demonstrating lupus pernio - purplish infiltration of the nose (& sometimes cheeks, ears, hands & feet). BHL suggests stage 1 sarcoidosis which now progressed. (stage 2: BHL & peripheral pulmonary infiltrates, stage 3: peripheral pulmonary infiltrates alone, stage 4: progressive pulmonary fibrosis, bullae, pleural involvement). Pts é BHL alone do not need Rx as most recover spontaneously, but parenchymal dis. (evident on clinical exam in this case), either symptomatic, static or progressive, is an indication for corticosteroid Rx. Severity of fibrosis ➜ Ix é CT thorax & lung function tests. Kveim tests are now obsolete in current practice. MRCP2 Dermatology Dr.Sherif Badrawy
- 24. 51.A violent local erythema blisters & recurs at the same site suggests a fixed drug eruption. A skin biopsy is Dx, eosinophilic infiltrate. 52.lnfliximab is a new biological Rxs, in RA, IBD & psoriasis & psoriatic arthritis. acts as anti- TNF-alpha antagonist & have a relatively good safety profile. The most important concern is re(+) TB. It is important to exclude TB before starting Rx. by a chest X-ray & either a Heaf or Mantoux test. 53.Behaet's syndrome is MC in young Turkish M & presents é recurrent oral & genital ulcers. It is also assoc. é eye problems eg Ant. & posterior uveitis & an asymmetrical migratory non- erosive oligoarthritis. Also neurological compliations, Esp. meningoencephalitis. Reiter's syndrome is triad of conjunctivitis, urethritis & arthritis. + erosions in the mouth & also on the penis where they are known as circinate balanitis. 54. Pemphigus is a gp of AI blistering dis. of the skin & mm. include pemphigus vulgaris (PV), pemphigus foliaceus & paraneoplastic pemphigus. PV is an AI, intraepithelial, blistering dis. affecting the skin & mucous membranes & is mediated by circulating autoAbs against keratinocyte cell surfaces. PV presents é oral lesions in the majority of Pts, & most Pts develop cutaneous lesions. The 1ry lesion of PV is a flaccid blister. The cause of PV is unknown but there is a recognised association é the human leucocyte Ag DR4 & human leucocyte Ag DRw6 alleles. Pts are often suffering from other AI dis., esp. MG & thymoma. DD for intraepidermal blistering: • friction • eczema . multilocular • infection • TEN. Causes of subepidermal blistering include : • burns • pemphigoid . ➜ tense, haernorrhagic, unilocular bullae which a↑ on abnormal(erythematous, urticated) skin. Mucosal involvement is uncommon. Nikolsky's Ss is -ve 55. This rash is typical of HSP. The Henoch-Schonlein syndrome includes polyarthralgia (but rarely true arthritis), bowel involvement (± abdominal pain in children) & renal involvement (focal necrotizing GN). In adults, up to 1/4 will develop RPGN & nephritic syndrome will occur in half of these Pts. 56. Acanchosls nigricans, MC assoc. with gastric adenocarcinoma. Other assoc. include obesity & DM. Coeliac dis. is assoc. é dermatitis herpetiformiss; Crohn's & ulcerative colitis are assoc. é erythema nodosum & pyoderma gangrenosum. MRCP2 Dermatology Dr.Sherif Badrawy
- 25. 57.This Pt already describes 3 criteria for SLE (> 4/ 11 are required to make Dx although these may be serially not necessarily simultaneously). A ↑ titre of dsDNA Abs is virtually exclusive to SLE & would confirm this Dx. Titres can be used to measure dis. activity alongside ESR & C3, C4 levels. CRP is not esp. useful in SLE as levels may remain ↓in active dis.. 58.pretibial myxoedema which occurs in 5% of Pts é Graves dis. almost always accompanied by exophthalmos & occasionally thyroid acropachy (finger clubbing). Nail pitting & onycholysis occur in psoriasis & onycholysis may also occur in thyroid dis., koilonychia in iron-deficiency anaemia, leukonychia é chronic liver dis. & hypoalbuminaemia 59. tuberous sclerosis é 'adenoma sebaceum', angiofibromata usu. affecting malar area & nasolabial folds. The hypopigmented areas are 'ashleaf macules', seen easily é a Wood's lamp ,shagreen patches (flesh·coloured leathery patches} & ungal fibromata seen in approximately 40% of Pts. The condition is assoc. é epilepsy Lichen planus (LP) characteristically affects flexor surfaces, esp. the wrists. fine white streaks on the surface of the MRCP2 Dermatology Dr.Sherif Badrawy
- 26. lesions (Wickham's striae) . It demonstrates the Koebner phenomenon (as does psoriasis)· a linear pattern along scratch marks or scars. There are often asymptomatic lacy white lesions in the buccal mucosa. Certain drugs may cause an LP·Iike eruption 60. Irritant contact dermatitis is the MC form of occupational skin dis. (up to 80%). Abrasives & cleaning agents (soaps, detergents & water < hand cleansers used by medical workers) & excessive exposure to water are common causes in predisposed individual - usu. a Hx of atopic dermatitis. Rx is prevention (avoidance of Irritant product/barrier creams etc) & Rx with topical CST & emollients. Patch test if there is uncertainty about the allergen but must be done in an unaffected area & 2 weeks after dermatitis has subsided. 61. erythema multiform& Stevens-Johnson syndrome. mucocutaneous drug-induced (sometimes idiopathic) reaction characterised by skin tenderness, erythema of skin & mucosa, fol↓ed by extensive epidermal necrosis & sloughing. Nicolsky's Ss is described. It is potentially life-threatening dt multi-system involvement. Early Dx & withdrawal of suspected drug(s) is very important. iv fluids/electrolytes ➜ as for Pts é 3rd-degree burns. Systemic steroids used early in dis. & no proven effect on morbidity & mortality. Only frankly necrotic skin ➜ debrided. 62.Erythema gyratum repens (EGR) is a paraneoplastic process. Characteristic concentric erythematous bands forming a wood·grain appearance help DD EGR from other erythemas, ex. erythema annulare centrifugum, erythema migrans, & erythema marginatum. EGR is assoc. é malignancy In up to 80% of Pts. lung cancer is the MC association, esp. in a Pt who is a smoker. also breast, bladder, cervical, stomach, & prostate cancer.Most Pts é EGR develop the eruption before the Sx of underlying malignancy. time interval may be up to 6 y.. EGR is assoc. é some non·malignant conditions, pulmonary TB, SLE, CREST 63.Gas gangrene is a medical emergency. Rapid onset of ms necrosis, gas production, & sepsis are the hallmarks of this dis.. dt exotoxin producing clostridial species (large, Gram +ve, spore- MRCP2 Dermatology Dr.Sherif Badrawy
- 27. forming bacilli), which are normally found in soil & the GIT. MC infection type is traumatic gas gangrene, occurs by direct inoculation of contaminated ischaemic wounds. Clostridium perfringens causes 80-95% of cases of gas gangrene. 64.Scleroderma is a rare multi·system chronic condition of unknown cause➜ tissue fibrosis, small BV vasculopathy (Raynaud's phenomenon) & autoimmunity. Diffuse scleroderma ➜ both cutaneous & visceral involvement, é rapid skin thickening on the extremities, face & trunk. limited scleroderma has a ↓er risk of early visceral involvement.no cure for scleroderma & Rx is aimed at aggressive Rx of symptoms. 65.Morphoea or localised scleroderma is a plaque of indurated mauve skin later becomes waxy & either pale or hyperpigmented é absent hair & sweating. Young adults 20 to 40 y. affected commonly. cause is unknown may be provoked by trauma or infection. Extensive morphoea may mimic systemic sclerosis, but differs in the absence of systemic dis., Raynaud's phenomenon & hand lesions. AutoAbs are usu. -ve. Plaque morphoea may improve spontaneously but local steroids, topical & oral vitamin D & light Rx can be used. 66.Drug hypersensitivity syndrome is a serious hypersensitivity reaction occur 3-6 weeks after certain drugs, esp. anticonvulsants and antimicrobials é fever, facial oedema, generalised papulopustular or exanthematous rash, lymphadenopathy, or hepatitis. sometimes assoc. é nephritis, pneumonitis, myocarditis & hypothyroidism é eosinophilia & mononucleosis. The drug hypersensitivity syndrome responds to oral steroid Rx. 67. Behaet's dis is largely a Dx of exclusion & can often be confused é Crohn's dis. ➜ the latter must be excluded. a systemic vasculitis of AAs & VVs é a tendency to thrombosis. > 90% of cases painful oral aphthous ulcers, > 70% genital aphthous ulcers & > 50% ocular inflammation. arthritis, CNS involvement & skin lesions e .g. erythema nodosum, folliculitis & acneiform lesions on the face. a relapsing & remitting course. Rx is symptomatic, & in the case of eye dis. is ↓ the progression of dis.. 68.The most likely Dx is of a BCC. MC non-melanoma skin malignancy. BCCs or rodent ulcers MC occur in middle-aged or elderly fair-skinned individuals é extensive sun exposure regardless MRCP2 Dermatology Dr.Sherif Badrawy
- 28. the form . Most occur on the face, but sometimes on the limbs & trunk. starts as a small translucent papule é obvious telangiectasia over the surface. gradually ↑ in size centre may ulcerate & crust. Rx is complete excision é a margin of normal skin. 69. Tinea cruris, ( jock itch) or ringworm of the groin, is a dermatophytoses is > men. transmitted via direct contact bw infected Pts & indirect contact é contaminated objects ex. towels, bed linens & clothing. affected area is sharply demarcated & a scaly ↑ red border spreads to inner thighs from the groin in a symmetrical fashion, but asymmetrically may occur. scrotum is usu. spared in distinct contrast é infections of this area by Candida. In acute infections, the rash may be moist and exudative & Pts may c/o of intense pruritus. Microscopic examination of (KOH) skin scraping is Dx & reveals the typical long branch-like structure of the fungus. if given a steroid cream will exacerbate the fungal infection. 70.Albinism is one of the general hypopigmentary dis. defect in production of pigment melanin. conditions fall into this classificationinclude oculocutaneous albinism types 1-4, ocular albinism, Chediak-Higashi syndrome, Hermansky-Pudlak syndrome & Griscelli syndrome. Oculocutaneous albinism type 1 complete absence of melanin in the hair, the skin & the eyes. Other problems é the eyes in these Pts photophobia, moderate to severe reduction in visual acuity & nystagmus. almost all of these Pts have iris transillumination defects & present é congenital motor nystagmus may be accompanied by ↓d visual acuity, refractive errors, fundus hypopigmentation, lack of foveal reflex & strabismus. Homocystinuria is an inherited AR defect dt defective methionine metabolism. have a typical physical appearance (long thin extremities, arachnodactyly, pale skin & hair), & unless the condition is Dx early & dietary restrictions started, Pts have other Ss of the dis. from early childhood. MRCP2 Dermatology Dr.Sherif Badrawy
- 29. Phenylketonuria is another inherited AR condition ➜ a defect in pathway of phenylalanine metabolism. routinely screened for at birth & appropriate dietary restrictions. The Pts are of fair hair & skin but the other clinical Ss of the disorder are mainly of historical interest. Note: Pts suffering from albinism may dye their hair & eyebrows so the Dx is not immediately evident, esp. if the Pt wears dark glasses to avoid the light hurting their eyes. 71. HSV type 1 is normally assoc. é orofacial infections. On the eyelids, it typically presents as a rash consisting of bw 3 & five vesicles on the eyelids may preceded by a prodrome of pain, tingling, burning or itching, usu. Lasts up to 6 h. eyelid may be oedematous, erythematous & the Pt may c/o of localised pain & tenderness. These vesicles become pustular or ulcerative é formation of crusts éin 72-96 h & heal over 8-10 days. important to ask if the Pt had a recent cold sore of the mouth or in contact é anyone who has a cold sore infection, since direct spread from the mouth to the eye can occur via contact é infected saliva. eye is also examined, both externally (the cornea looking for classic dendritic ulcer on the surface) & internally (exclude acute retinal necrosis, a very rare complication of HSV infection may ➜blindness). 72. Oral leukoplakia ➜ a white patch cannot be rubbed off - it is a Dx of exclusion. a potentially malignant condition & > common in men. patches are white & well defined. Pts tend not to be symptomatic. Causes include smoking, alcohol consumption, ill-fitting dentures & malocclusion of teeth. Oral lichen planus appears as patches of fine white lines & dots. The white sponge naevus of Canon is a white folded dysplasia of the mm. a familial condition é an AD inheritance. Aphthous ulcers are painful & hence the Pts are symptomatic. 73. Dermatitis artefacta is a condition where the skin lesions are inflicted by the Pt on themselves. It may be dt an underlying psychological problem, a form of emotional release from distressful situations, or attention-seeking behaviour esp. when the Pt is lonely. > common in women than in men. lesions have unusual shapes ± a linear or geometric pattern. Clearly demarcated from surrounding skin & usu. appear overnight. Different methods may be used to injure the skin (nails, caustic soda, cigarettes). lesions are on exposed skin & readily accessible to the Pt's hands. MRCP2 Dermatology Dr.Sherif Badrawy
- 30. 74.Pityriasis rosea is an acute exanthem initially presents é a 1ry plaque (herald patch) fol↓ed, 1- 2 weeks later, by a generalised rash which can last up to 6 weeks. Prodromal Sx may precede the herald patch & pruritus may be intense. The herald patch measures 1-2 cm in diameter & is usu. Located on the trunk. The 2ry rash is symmetric & again localised to the trunk & the adjacent areas of the neck & limbs. The rash has a Christmas tree pattern. Pityriasis alba is a hypopigmented dermatitis primarily in school-aged children who are symptomatic. 1/2 cases, lesions are limited to the face. Pityriasis versicolor (tinea versicolor) is a superficial cutaneous fungal infection ➜ macules on the chest & the back. It is dt Malassezia furfur. The main c/o of affected Pts tends to be abnormal pigmentation, which is cosmetically upsetting, & mild pruritus. 75. rash in a scar or in the site of an injury is known as Koebner's phenomenon. usu. appears around 7 to 14 days after the injury. Skin disorders show this reaction include psoriasis, lichen planus and vitiligo. The Koebner response occurs in up to 20% of Pts é psoriasis. The term pseudo Koebner is used for conditions ex. molluscum contagiosum & viral warts where the phenomenon a↑from the spread of an infective agent. The reverse Koebner also exists where trauma to a lesion ➜it resolving. 76. Erythroderma is the term of any inflammatory skin dis. if Affects > 90% of the body surface. often accompanied é fever, shivering and malaise. eczema & psoriasis are MCC. Other MRCP2 Dermatology Dr.Sherif Badrawy
- 31. ppt lymphoma, drugs & pityriasis rubra pilaris. It’s often assoc. with metabolic disturbances, & Pts may develop hypothermia or ↑output cardiac failure. Rx in hospital é monitoring of fluid balance and temp.. may continue for months or y. & may also relapse. 77. lsotretinoin is the most clinically effective Rx for acne, & usu. Produces long-term remission. ↓s ↑ sebum production, comedogenesis & colonisation é Propionibacterium acnes. prescribed for Pts é moderate acne who are failing to respond to conventional Rx. many SEs. Esp. very teratogenic. A -ve pregnancy test must be obtained before Rx, & counselling must be given regarding contraception. LFTs & lipids ➜ checked in Pts as these usu. become ↑ é Rx. Pts generally c/o of dryness of the mouth & lips, & ➜ advised to use regular moisturisers. 78. In M, the back is the MC area to develop a melanoma, while in women the legs are MC affected. The location does not affect prognosis. The recognition of Ss of malignancy in a pre- existing lesion depends on assessment of asymmetry, border, colour, diameter & ↑. The darkening of this gentleman' s lesion prompted the subsequent excision & Dx.The thickness of the melanoma, or Bres↓er thickness, is the single most important prognostic feature & impacts of Rx decisions. 79. Orogenital sex poses a ↓risk for HIV transmission but it is a common route of syphilis acquisition. 2ry syphilis usu. commences 4-10 weeks after the 1ry chancre (which can commonly occur in the oral cavity), but the 2 stages are sometimes concurrent. Pts usu. present é maculopapular rashes affecting the entire trunk, but any form of lesion may occur. Alopecia is well recognised as are multiple painless aphthous ulcers. Sore throat, myalgia, fever & Wt loss are common to both conditions. 80. Granuloma annulare presents as a ring of small smooth papules, which enlarge centrifugally. Lesions may be solitary or multiple & usu. present on the hands and feet. They are usu. asymptomatic. They occur MC in individuals under the age of 30 y., & are > common in women than in men. association é DM.± association é HIV infection. Clinically, lesions lie over the knuckles & are composed of dermal nodules into a rough ring shape. On the trunk many lesions ± a purple tinge to them. Lesions usu. resolve over 2-3 y.. Stubborn lesions respond to intralesional trimacinolone or systemic immunosuppressants. MRCP2 Dermatology Dr.Sherif Badrawy
- 32. 81.Psoriasis is often difficult to recognise & DD from tinea & eczema in the genitalia. There are often skin changes elsewhere. The erythematous scaling plaque is clinically Dx. In the groin it is often not scaly but glistening & well demarcated. The Rx is moderately potent topical steroids in the 1st instance. 82. lupus vulgaris dt mycobacterium TB infection. It is a chronic TB of the skin. It is exceedingly rare these days. Rx is the same as for pulmonary TB. BCC & SCCs become infiltrated will be ulcerated andc do not progress so rapidly. lupus pernio occurs in Pts é sarcoid commonly those of African-Caribbean origin. It is usu. mauve/purple in colour. Cutaneous leishmaniasis occurs after a flu-like illness when Pts develop papules which can ulcerate on the trunk. The incubation time is 7 days to a few months. 83. Necrolytic migrating erythema is an erythema é a moving crusted edge. present, usu. é anaemia, stomatitis, Wt loss & DM, it signals the presence of a rare glucagon-secreting tumour of the pancreas. In alcoholics however, nutritional deficiencies cause many overlapping Sx making the Dx difficult. MRCP2 Dermatology Dr.Sherif Badrawy
- 33. 84.Early necrobiosis lipoidica diabeticorum is often difficult to Dx dt is psoriatic in nature & telangiectasia are seen on the waxy surface. Lesions appear as one or > discoloured areas on the fronts of the shins, shiny, atrophic & brown-red or slightly yel↓. The margin may be erythematous or violet. Minor injury can be s↓erto heal. 85. Phototoxicity has been described for all quinolones including ciprofloxacin. PCT could account for the blisters, but Pts tend to have other skin Ss e.g. blisters, erosions & milia on exposed parts of the face & backs of the hand in response to sunlight. Polymorphic light eruption affects all exposed areas & often ➜blistering e.g. on the face. It is usu. preceded by a long Hx of sun intolerance. 86. lichen planus in Caucasians are small, mauve flat-topped, shiny papules which sometimes have white streaky areas on the surface (Wickham's striae). characteristically occur on the flexor aspect of the wrist but are often widespread on the trunk & limbs & may occur at sites of trauma. As the rash gets better the papules will change colour from purple to brown. The rash tends to last 9-12 months before disappearing. In type V skin however, the lesions look different & often hyperpigmented. The residual post-inflammatory hypopigmentation occurs dt scratching. It is often a difficult Dx to make in these Pts. MRCP2 Dermatology Dr.Sherif Badrawy
- 34. 87.This Pt has recurrent cellulitis 2ry to herpetic whit↓, a self-limiting dis. Young adults are typically affected by HSV-2 where a prodroma up to 72 his fol↓ed by a recurrence of 7-10 days' duration. Lymphangitis and lymphadenitis 2ry to HSV infection is a recognised complication. Lymphoedema of the hand & forearm may rarely develop. Acute infection ➜ Rx with ↑ dose oral aciclovir fol↓ed by ↓er doses as prophylaxis. Although this is not common it is very important to remember in cases of unexplained recurrent cellulitis. MRCP2 Dermatology Dr.Sherif Badrawy