Phemphigus
•Download as PPTX, PDF•
101 likes•55,017 views

this topic is on phemphigus vulgaris. describes in detail regarding the phemphigus, its causes, pathophysiology, management and nursing care plan

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (14)
Similar to Phemphigus
Similar to Phemphigus (20)
More from Siva Nanda Reddy
More from Siva Nanda Reddy (20)
Recently uploaded
Recently uploaded (20)
Phemphigus
- 1. Phemphigus By: Mr. M. Sivananda Reddy
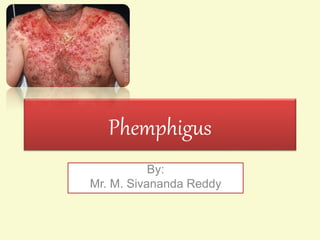
- 2. Definition Pemphigus is a blistering autoimmune disease that affects the skin and mucous membranes.
- 4. Etiology: • Autoimmune disease involving immunoglobulin G. • Genetic factors may also play a role in its development, with the highest incidence among those of Jewish or Mediterranean descent. • Usually occurs in men and women in middle and late adulthood. • May be associated with Penicillins and Captopril and with Myasthenia Gravis.
- 5. Pathophysiology • Pemphigus antibody is directed against a specific cell-surface Antigen (Desmoglein) in epidermal cells. • A blister forms from the antigen–antibody reaction.
- 6. Types There are three types of pemphigus which vary in severity: • Pemphigus vulgaris • Pemphigus foliaceus • Paraneoplastic pemphigus.
- 7. • The most common form of the disorder is pemphigus vulgaris . It occurs when antibodies attack Desmoglein 3 (a protein that is present in the epidermal layer of skin). • Pemphigus foliaceus (PF) is the least severe of the three varieties. Desmoglein 1, the protein that is destroyed by the autoantibody
- 8. • The least common and most severe type of pemphigus is paraneoplastic pemphigus (PNP). This disorder is a complication of cancer
- 9. Clinical Manifestations • oral lesions appearing as irregularly shaped erosions that are painful, bleed easily, and heal slowly. • The skin bullae enlarge, rupture, and leave large, painful eroded areas that are accompanied by crusting and oozing
- 10. • A characteristic offensive odor emanates from the bullae and the exuding serum. • Nikolsky’s sign: The Nikolsky sign is dislodgement of intact superficial epidermis by a shearing force.
- 11. Complications • Secondary bacterial infection • Fluid and electrolyte imbalance • Hypoalbuminemia
- 12. Management The goals of therapy are • To bring the disease under control as rapidly as possible • To prevent loss of serum and the development of secondary infection • To promote re-epithelization
- 13. • Corticosteroids are administered in high doses to control the disease and keep the skin free of blisters. • In some cases, corticosteroid therapy must be maintained for life.
- 14. • Immunosuppressive agents (eg, Azathioprine, Cyclophosphamide) may be prescribed to help control the disease and reduce the corticosteroid dose. • Plasmapheresis (ie, plasma exchange) temporarily decreases the serum antibody level and has been used for life-threatening cases.
- 15. NURSING DIAGNOSES • Acute pain of skin and oral cavity related to blistering and erosions • Impaired skin integrity related to ruptured bullae and denuded areas of the skin • Anxiety and ineffective coping related to the appearance of the skin and no hope of a cure • Deficient knowledge about medications and side effects
- 16. Nursing interventions • Meticulous oral hygiene is important to keep the oral mucosa clean and allow the epithelium to regenerate. • Frequent rinsing of the mouth is prescribed to rid the mouth of debris and to soothe ulcerated areas. • The lips are kept moist with lip balm
- 17. • Cool wet dressings are protective and soothing. • The patient with painful and extensive lesions should be pre-medicated with analgesics before skin care is initiated. • Hypothermia is common, and measures to keep the patient warm and comfortable are priority nursing activities
- 18. • After the patient’s skin is bathed, it is dried carefully and dusted liberally with non-irritating powder, which enables the patient to move freely in bed.
- 19. Reducing anxiety of the patient: • The patient is encouraged to express freely anxieties, discomfort, and feelings of hopelessness. • Arranging for a family member or a close friend to spend more time with the patient can be supportive. • Referral for psychological counseling may assist the patient in dealing with fears, anxiety, and depression.
- 20. Prevention of infection: • The skin is cleaned to remove debris and dead skin and to prevent infection • The oral cavity is inspected daily, and any changes are reported. • Assess for signs and symptoms of local and systemic infection.
- 21. • Antimicrobial agents are administered as prescribed, and response to treatment is assessed. • Health care personnel must perform effective hand hygiene and wear gloves. • In the hospitalized patient, environmental contamination is reduced as much as possible. • Protective isolation measures and standard precautions are warranted.
- 22. • Blood component therapy may be prescribed to maintain the blood volume, hemoglobin level, and plasma protein concentration. • Serum albumin, protein, hemoglobin, and hematocrit values are monitored.
- 23. • The patient is encouraged to maintain adequate oral fluid intake. • Cool, non-irritating fluids are encouraged to maintain hydration. • Small, frequent meals or snacks of high-protein, high calorie foods help maintain nutritional status. • Parenteral nutrition is considered if the patient cannot eat an adequate diet.