2. INTRODUCTION
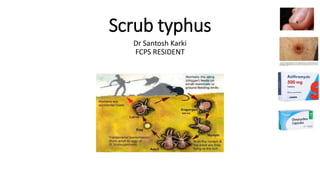
• Scrub typhus is a mite-borne infectious disease caused by Orientia
tsutsugamushi (previously called Rickettsia tsutsugamushi).
• Scrub typhus is of greatest public health importance in the rural Asian
tropics.
• Scrub typhus is manifested clinically by high fever, cough, intense
generalized headache, diffuse myalgias, and, in many patients, rash
and an eschar at the site of the insect bite
3. MICROBIOLOGY
• O. tsutsugamushi is an obligate intracellular, gram-negative
coccobacillus that infects a range of host cell types including
endothelial cells, monocytes, macrophages, and dendritic cells.
• Like all rickettsiae, O. tsutsugamushi cannot be propagated in cell-free
media
• It is unique in that it is released from infected cells by budding from
the plasma membrane of host cells
7. CLINICAL MANIFESTATIONS
• Clinical manifestations can range from mild signs and symptoms to multiorgan
failure and death
• Acute febrile illness — Infection commonly presents as an acute febrile illness
about a week after the bite of an infected mite, although clinical onset can range
from 6 to 21 days after exposure
• Scrub typhus may begin insidiously with headache, anorexia, and malaise, or start
abruptly with chills and fever. As the illness evolves, most patients develop the
following symptoms:
• ●Fever, which typically lasts for long periods in untreated patients (median 14.4
days; range 9 to 19) [8]
• ●Intense generalized headache
• ●Diffuse myalgias
• Rash, eschar, and other signs and symptoms may also be present
8. Other signs and symptoms
Lymphadenopathy Localized, and subsequent generalized lymphadenopathy, occurs in the majority of patients and may
be accompanied by inflammation of the lymphatic sinuses, splenomegaly, and portal triaditis.
Gastrointestinal
Nausea, vomiting, and/or diarrhea are prominent findings in approximately one-fourth of patients
Respiratory Respiratory complaints occur in up to two-thirds of cases, with symptoms ranging from mild cough
to overt acute respiratory distress syndrome (ARDS)
Cardiovascular Relative bradycardia occurs commonly in patients with scrub typhus . Relative bradycardia has been
defined as a median increase in heart rate <10 beats/min per 1ºC increase in temperature
Central nervous
system
Meningitis, meningoencephalitis, seizures, and strokes, especially in children and older adults
Altered sensorium is particularly common in older patient
Renal Acute kidney injury has been reported in those with severe disease
9. Laboratory findings
• Most patients with severe illness develop thrombocytopenia.
Elevations in hepatic enzymes, bilirubin, and creatinine may also be
present
• Leukopenia or leukocytosis can occur, but most have a normal white
blood cell count
10. DIAGNOSIS
• Initial diagnosis of scrub typhus is made presumptively, based on
compatible clinical signs, symptoms, and laboratory features as well
as epidemiologic clues
• Treatment should be initiated immediately when the diagnosis is
suspected
• A rapid response to empiric treatment can also be used to support
the diagnosis, although response times >48 hours have been reported
11. Diagnostic tests
DIAGNOSTIC TEST REMARKS
SEROLOGY Indirect fluorescent antibody (IFA) test remains the mainstay of serologic diagnosis.
Detectable IgM antibodies when combined with an appropriate clinical syndrome and
epidemiology
A dot blot immunoassay dipstick, which is undergoing clinical evaluation, may permit rapid
diagnosis of scrub typhus
Biopsy of an eschar or
generalized rash
In challenging cases
pathological hallmark of scrub typhus is a lymphohistiocytic vasculitis
Polymerase chain reaction PCR testing of blood samples even in the minority of patients who lack IgM antibodies early
in the course of infection
PCR assays on blood have demonstrated lower sensitivity than specificity
Culture Culture of this organism is available in only a few specialized laboratory centers with rigorous
quality control and appropriate laboratory safety measures.
13. TREATMENT
• Indications
• All patients with suspected or confirmed scrub typhus should be
treated with antimicrobial therapy.
• Treatment should be initiated as soon as possible.
• Delayed administration of antibiotics has been independently
associated with the development of major organ dysfunction and
hospitalization for >10 days
14. Determining disease severity
Types Clinical Features
Mild Patients with mild to moderate disease typically present with fever, myalgia, and headache
Moderate Patients with mild to moderate disease typically present with fever, myalgia, and headache as well as
a rash (with or without eschar) and/or cough.
Severe Combination with clinical or laboratory manifestations that indicate end-organ damage.
These include hyperbilirubinemia, renal failure, cardiovascular collapse (hypotension/shock), acute
respiratory distress syndrome (ARDS), and meningoencephalitis.
15. • Preferred antimicrobial regimens
For patients with presumed mild to moderate scrub typhus, we suggest
monotherapy with doxycycline or azithromycin.
• Persons with severe disease
Monotherapy with doxycycline is standard care
200 mg of doxycycline twice daily on day one, followed by 100 mg twice
daily for a total duration of seven days
However, combination therapy with doxycycline and azithromycin may be
considered on a case-by-case basis.
Duration : doxycycline -7 days , azithromycin 5-7 days
16. Alternate antimicrobial regimens
• Rifampin
Contraindications to doxycycline and azithromycin (the preferred agents)
rifampin creates challenges with its many drug-drug interactions
rifampin (600 mg once daily for five days)
Combination therapy with doxycycline plus rifampin is rarely indicated
• Fluoroquinolones
particularly in mild/moderate disease
associated with delayed time to resolution and higher mortality compared to doxycycline or minocycline
• Chloramphenicol
first drug
no significant differences in time to resolution of fever and incidence of relapse in patients treated
with doxycycline or chloramphenicol
• toxicity of this drug and difficulty obtaining it in most countries, chloramphenicol should be reserved
for situations when other options are not available.
17. Considerations during pregnancy
• Scrub typhus may cause spontaneous abortions or stillbirths in
pregnant persons
• Typically administer azithromycin (500 mg daily) for seven days
18. PREVENTION
• Prevention of scrub typhus consists of avoiding exposure to mites
• No vaccine is available to prevent the transmission of scrub typhus