3. Definition
• The term receptor is used in pharmacology to
denote a class of cellular macromolecules that
are concerned specifically and directly with
chemical signaling between and within cells.
4. • Affinity:
– The capability of a drug to form the complex (Drug
Receptor Complex) with its receptor.
• Intrinsic activity:
– The ability of a drug to trigger the pharmacological
response after making the drug-receptor complex.
D + R DR
D: Drug or endogenous ligand
R: Receptor
DR: Drug-Receptor Complex
5.
6.
7. • Agonist:
– These are the drugs which have both high affinity
as well as high intrinsic activity.
• Antagonist:
– These are the drugs which have only the affinity
but no intrinsic activity.
8.
9. When two drugs are binding to the same receptor
and at the same site, why is it that one is acting
as an agonist while other is serving as an
antagonist...?
10. The concept of dual nature of receptors
• Receptors usually exists in two conformations
– The active (Ra) state
– Inactive (Ri) state
If Ra and Ri conframations are in equlibrium, the
extent to which this equilibrium perturbed shall be
determined by the relative affinity of the drug for
these two conframations
11. • Agonist:
– These drugs have high affinity for the active
conformation (Ra) than for inactive (Ri)
• Antagonist:
– These drugs bind to either of these conformations
(Ra & Ri) with equal affinity.
• It will not shift the equilibrium to any side
12. Partial agonist
– These have slightly higher affinity for Ra than for
Ri and hence shift the eaulibrium toward Ra to a
lesser extent than true agonist.
– Such drugs therefore display an intermediate
effectivesss between the agonist and antagonist
13.
14. Inverse agonist
• There are certain receptors which remain
inherently in the Ra state even in the absence of
an endogenous ligand or an exogenous agonist.
• Inverse agonists inactivate such constitutively
active receptors and therefore prevent its basal
activity.
• As a result inverse agonist produce an effect
opposite to that of an agonist / drug even in its
absence.
15.
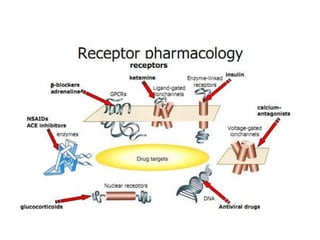
16. Receptor Types
1. Ion-channel Receptors (Ionotropic Receptors)
2. G-Protein Coupled Receptors (Metabotropic
receptors)
3. Kinase-linked Receptors
4. Intracellular Receptors (Cytosolic Receptors)
5. Enzymes as Receptors
6. Drugs which act through Modulation of Voltage
Gated Ion Channels (Voltage-Operated
Channels)
17.
18. Ion-channel
• Localised on the cell membrane
• Coupled directly to an ion channel
• It is a channel with a receptor site.
• Agonists opens the channel.
• Antagonists prevents agonist from opening the
channel
• Inverse agonist closes an open channel
19. • Multiple subunit proteins which form cation
or anion channels
• Channel properties are determined by the
composition of subunit isoforms
– agonist affinity
– ion permeabilities
– conductance properties
– activation and deactivation times
– desensitisation kinetics
• Activity can be regulated by varying
composition of different subunits
20. Two main families
1. Nicotinic receptor family (include nACh
receptors, GABAA, GABAC, glycine receptors
and the 5-HT3 receptor)
2. Glutamate receptor family (several different
receptor types classified into NMDA
receptors and non-NMDA receptors)
21.
22.
23. G-Protein Coupled Receptors
• GPCRs are composed of 7 transmembrane
helices which have an extracellular domain as
drug or neurotransmitter binding site and an
intracellular domain that couples to G-protein
24.
25.
26. Why do GPCRs not act directly on
effectors?
1. Means of amplifying signal
2. G proteins can act as integrators of inputs
from several stimuli (convergence)
3. G proteins can regulate more than one
effector (divergence)
27.
28. Three main variants of GPCRs
1. Gs: Stimulation of Adenyl cyclase
2. Gi: Inibition of Adenyl cyclase
3. Gq: Controls phospholipase-C activity
29. G-Protein coupled effector system
1. Adenylate cyclase-cAMP system
2. Phospholipase-C-inositol phosphate system
3. Ion channels
33. Kinase-linked Receptors
• These receptors are directly linked to:
1. Tyrosine kinase (e.g. receptors for insulin and
various growth factors)
Or
2. Guanylate cyclase (e.g. receptors for atrial
natriuretic peptide)
34.
35. Intracellular Receptors
This nuclear receptor family senses signals from
the lipid soluble substances (e.g. Vit A & D) and
other hormonal substances to influence the gene
expression.
36.
37.
38. Enzymes as Receptors
• Drugs can either mimic the enzyme’s substrate
or may bind to its allosteric site to produce the
effect
E.g.
Angiotensin-converting enzyme
Acetylcholinesterase enzyme
39. Voltage-Operated Channels
• VOC’s like ROC’s are ion channels that are
gated only by voltage.
• While ROC’s assume only 2 states: Open or
Close; VOC’s also assumes a third state called
‘refractory’ (inactivated) state.
40. Refractory State
• In this state the channel is unable to ‘open’ (or
reactivate) for a certain period of time even
when the membrane potential returns to a
voltage that normally opens or activates the
channel.
• State Dependent Binding
41.
42.
43.
44. Down-regulation of Receptors
• Prolonged exposure to high concentration of
agonist causes a reduction in the number
receptors available for activation.
• This results due to endocytosis or
internalisation of the receptors from the cell
surface
45. Up-regulation of Receptors
• Prolonged occupation of receptors by a blocker
leads to an increase in the number of receptors
with subsequent increase in receptor
sensitivity.
• This is due to externalisation of the receptors
from inside of the cell surface.
46. Spare Receptors
• A drug can produce the maximal response
when even less than 100% of the receptors are
occupied. The remaining unoccupied receptors
are just serving as receptor reserve are called
spare receptors
47.
48.
49. Receptor Related Diseases
• Myasthenia Gravis:
– Antibodies against the cholinergic nicotinic receptors
at motor end plate.
• Insulin Resistant Diabetes
• Testicular feminisation
• Familial Hypercholesterolaemia