Scaphoid fracture and hcs
•Download as PPT, PDF•
7 likes•2,735 views

managing scaphoid fractures

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Scaphoid fracture and hcs
Similar to Scaphoid fracture and hcs (20)
More from Vaikunthan Rajaratnam
More from Vaikunthan Rajaratnam (20)
Recently uploaded
Recently uploaded (20)
Scaphoid fracture and hcs
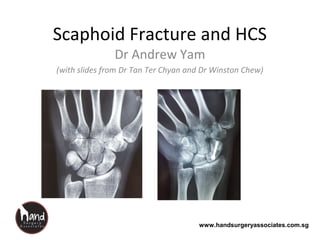
- 1. www.handsurgeryassociates.com.sg Scaphoid Fracture and HCS Dr Andrew Yam (with slides from Dr Tan Ter Chyan and Dr Winston Chew)
- 2. www.handsurgeryassociates.com.sg Role of the scaphoid • Link between proximal and distal carpal rows • Essential for carpal stability and normal carpal movement
- 3. www.handsurgeryassociates.com.sg Force transmitted from Distal carpal row via scaphoid to proximal carpal row during flexion/extension and radial/ulnar deviation Courtesy of Marc Garcia-Elias
- 4. www.handsurgeryassociates.com.sg Courtesy of Marc Garcia-Elias
- 5. www.handsurgeryassociates.com.sg Anatomy of scaphoidAnatomy of scaphoid Distalpole Distalpole Waist Waist Proximal poleProximal pole Scaphoid tuberosityScaphoid tuberosity
- 6. www.handsurgeryassociates.com.sg Retrograde blood supply toRetrograde blood supply to proximal poleproximal pole poor vascularitypoor vascularity Poor VascularityPoor Vascularity 70-80% of70-80% of blood supplyblood supply 20-30% of20-30% of blood supplyblood supply
- 7. www.handsurgeryassociates.com.sg Scaphoid fractureScaphoid fracture Most common carpal bone fracture • 60% (Hove, Scand J PRSHS 1999) to 79% (Smith, Cooney, JHS 1989) of isolated carpal bone fractures T a b l e O F I N C I D E N C E O F C A R P A L F R A C T U R E S Bone Number % of Total Scaphoid 5036 78.8 Triquetrum 880 13.8 Trapezium 144 2.3 Hamate 95 1.5 Lunate 92 1.4 Pisiform 67 1.0 Capitate 61 1.0 Trapezoid 15 0.2 6390
- 8. www.handsurgeryassociates.com.sg Epidemiology • Male • Young (peak incidence 2nd to 3rd decades) • Sporting injuries (football), motorcycle road traffic accidents, fall from heights
- 9. www.handsurgeryassociates.com.sg Pathomechanics of fracture • Frykman ; pathomechanics of distal radius fractures - hyper-extension and radial deviation = scaphoid # - lesser extension and lesser force = DR# • Weber, Chao 1978 - Wrist extension beyond 95 degrees - Radial deviation beyond 10 degrees LockedLocked IntoInto fossafossa BeyondBeyond normalnormal limitlimit # in# in tensiontension
- 10. www.handsurgeryassociates.com.sg Diagnosis of scaphoid fracture • History of fall on outstretched hand • Tenderness and swelling in anatomical snuffbox • XR – scaphoid views • CT scan • MRI scan
- 11. www.handsurgeryassociates.com.sg • 75% waist • 25% proximal pole • 5% distal pole Location of fracture
- 12. www.handsurgeryassociates.com.sg X-rays False negative rate of initial x-rays: 2-25% Supinated obliqueSupinated oblique Pronated obliquePronated oblique LateralLateral PAPA Scaphoid viewScaphoid view If not seen on x-ray done on day of injury, repeat the X-ray in 2 weeks or send for CT/MRI scan for early diagnosis Tuberosity Distal pole Distal third Waist Proximal pole
- 13. www.handsurgeryassociates.com.sg X-rays – other things to look out for • Scapholunate angle (lateral) • Intra-scaphoid angle (lateral/hyper-pronated view) • Scapholunate interval (concurrent SL injury) • Other carpal bone fractures • Concurrent perilunate dislocation • Concurrent distal radius fracture
- 14. www.handsurgeryassociates.com.sg CT scans • Early accurate detection of undisplaced fractures • Assess humpback deformity • Accurate measurement of intra-scaphoid angle • Planning tool for bone grafting procedure • Assess healing (cortical bridging)
- 15. www.handsurgeryassociates.com.sg MRI • Early detection of occult fractures within 24 hours of injury • Demonstrate vascularity of proximal pole (Gd enhanced study) – Low signal T1, low/high T2 signal: poor vascularity/AVN •Shows concurrent ligamentous injuries Coronal FSTIRCoronal FSTIRCoronal T1 FSECoronal T1 FSE
- 16. www.handsurgeryassociates.com.sg Russe classification 1960 Relatively stableRelatively stable heal in 6-12 weeksheal in 6-12 weeks With immobilsationWith immobilsation Relatively UNstableRelatively UNstable Longer timeLonger time
- 17. www.handsurgeryassociates.com.sg TJ Herbert classification 1984 • Fracture classification according to stability and chronicity • Stable - occult - incomplete - complete, undisplaced • Unstable - complete and displaced (>1mm) - comminuted - dislocated - proximal pole - other associated ligamentous injury
- 18. www.handsurgeryassociates.com.sg The Natural History – Scaphoid Fractures (treated) • ~90% unite with conservative treatment (NJ. Barton, JBJSB 2004) • >90% union rates following ORIF of acutely displaced fractures (Scott H. Kozin Hand Clin 2001) • 96% union in undsiplaced fractures and 88% displaced fractures (Cooney, Linscheid, Dobyns; Symposium on The Wrist; Orth Clin N. America 1984) • Non-union in approximately 5% of treated scaphoid fractures (Mack, JBJSA 1984) and in an unknown number of unrecognized fractures
- 19. www.handsurgeryassociates.com.sg The Natural History – Malunited Scaphoid Fractures • The Late Consequence of Scaphoid Fractures - NJ. Barton, JBJSB 2004 - Amadio 1989: Intrascaphoid angle >35 degrees had 27% satisfactory clinical and functional outcome, <35% had 83% good outcomes - Jiranek 1992: compared acceptable union (13) and those with >45 degrees (13) intra- scaphoid angle >> movement and strength were significantly affected The restoration of anatomic alignment results in better outcomes over the long term
- 20. www.handsurgeryassociates.com.sg Scaphoid Fractures • 5% of patients with united scaphoid fractures develop radio-carpal arthritis within 7 years
- 21. www.handsurgeryassociates.com.sg SNAC Wrist • Review of 46 patients with symptomatic scaphoid fracture non-unions
- 22. www.handsurgeryassociates.com.sg • Injuries to the scapho-lunate ligament or scaphoid fractures disrupt the intercalation between the scaphoid and the lunate • This results in flexion of the scaphoid with changes in the radio-scaphoid articulation
- 23. www.handsurgeryassociates.com.sg SNAC Wrist • Cystic changes in the scaphoid with sclerosis of the fracture ends Stage 1
- 24. www.handsurgeryassociates.com.sg SNAC Wrist • Degenerative changes in the radio-scaphoid joint Stage 2
- 25. www.handsurgeryassociates.com.sg SNAC Wrist • Loss of carpal height, pan-carpal arthritis Stage 3
- 26. www.handsurgeryassociates.com.sg Management of acute scaphoid fracture Casting •STABLE and UNDISPLACED fractures – 90% union rate •Cast duration guidelines (Gellmen JBJSB 1989): - distal = 8 to 10 weeks below elbow - waist = 6/52 above elbow, 6/52 below elbow - proximal = 6/52 above elbow, up to 6/12 below elbow • Proper assessment for union can be difficult – use CT scan
- 27. www.handsurgeryassociates.com.sg Surgical Treatment • Strong indications – displaced or unstable fracture pattern – all proximal pole fractures – Concurrent ligament injuries (Perilunate injury) or distal radius fracture requiring fixation • Relative indication – Patient preference for fixation instead of prolonged immobilization in cast
- 28. www.handsurgeryassociates.com.sg Early Internal Fixation of Scaphoid Fractures Should Acute Scaphoid Fractures Be Fixed? A Randomized Controlled Trial. JJ Dias, Wildin, et al. JBJSA October 2005 • Double arm; ORIF 44, casting 44 (8 weeks) • Matched for demographics, fracture type/displacement/deformity/comminution • ORIF – less nonunion (0% vs 25%) at 12 weeks – 30% minor complications – faster return to function – better grip strength, range of motion and satisfaction at 8 weeks
- 29. www.handsurgeryassociates.com.sg Early Internal Fixation of Undisplaced Scaphoid Fractures Minimally Invasive Fixation vs. Conservative Treatment of Undisplaced Scaphoid Fractures: A Cost Effectiveness Study. Papaloizos JHSB 2004 • Retrospective, two study groups; 23 operative, 62 conservative • Professions equally distributed, similar demographics • Outcome: operative group less costly to treat than conservative group (costs incurred in lost manhours) • Conclusion: operative treatment of scaphoid fractures is initially more expensive than conservative treatment but markedly decrease work compensation costs Fracture of the carpal scaphoid. A propsective randomized 12-year follow up comparing operative and conservative treatment. Saden JBJS 2001 • Conclsuion: operative treatment allows earlier return to function
- 30. www.handsurgeryassociates.com.sg Headless Compression Screw (HCS) fixation • Differential pitch in proximal and distal threads create compression force across fracture site • Cannulated screw facilitates percutaneous fixation with guide wire
- 31. www.handsurgeryassociates.com.sg Percutaneous HCS fixation Advantages Bone healing quicker than casting Avoids immobilisation Preserves palmar ligament complex, and local vascularity Indications Undisplaced or minimally displaced fracture
- 32. www.handsurgeryassociates.com.sg Palmar Percutaneous HCS Undisplaced or minimally displaced fractures of the waist and distal 1/3 of the scaphoid.
- 33. www.handsurgeryassociates.com.sg Dorsal Percutaneous HCS Proximal pole and proximal waist fractures
- 34. www.handsurgeryassociates.com.sg Open volar approach Displaced, irreducible or comminuted fractures in distal 2/3 Correction of humpback deformity with bone graft
- 36. www.handsurgeryassociates.com.sg Open Dorsal Approach Proximal pole fractures Vascularised bone graft for AVN
- 39. www.handsurgeryassociates.com.sg Technical considerations of HCS fixations Screw should be as close as possible along the central axis of scaphoid AND as perpendicular as possible to fracture line Make sure that the threads at the near end of the screw are fully buried in the bone at the insertion site. - always minus 4-6mm from measured length to make sure screw is not too long Make sure that all threads on the far side have crossed the fracture to ensure interfragmentary compression.
- 40. www.handsurgeryassociates.com.sg Complications of HCS • Screw too long Protruding screw STT or radioscaphoid joint impingement • Screw too short inadequate stability loosening and nonunion • Inadequate fracture reduction Malunion • Fracture distraction non-union
- 41. www.handsurgeryassociates.com.sg Scaphoid plate to salvage failed HCS fixation • Anatomical plate • 1.5mm variable locking • Indications – Comminuted fractures – Nonunion with previous screw tracks
Editor's Notes
- The scaphoid is the most complex carpal bone, making up the base of the lateral (mobile) column of the wrist (Navarro). It lies obliquely at about 45 degrees to the longitudinal axis of the two carpal rows. Most of its surface is made up of articular cartilage. Distally, it articulates with the trapezium and trapezoid in a gliding motion, The articulation with the trapezium forms a base for independent movement of the thumb. On the ulnar side, it articulates distally with the capitate, and proximally with the lunate in a rotary motion. Proximally, its large, biconvex surface allows articulation with the radius
- Grettve, Minne, Taleisnik & Kelly showed 3 principal arterial groups supplying the main body of the scaphoid VOLAR DORSAL DISTAL Recent studies by Gelberman & Menon suggested 2 vascular systems : volar & dorsal But whichever the study, may be simply semantics as more importantly, All the studies show POOR BLOOD SUPPLY to PROXIMAL POLE Cf abundant supply to distal 2/3 of scaphoid Prox pole, entirely intraarticular & completely covered with hyaline cartilage Negligible or non-existent independent blood supply Relies on intraosseous blood flow
- Frykman first showed that cadaver specimens were more likely to # scaphoid when wrist was HYPEREXTENDED AND RADIALLY DEVIATED If extensions angles less, more likely to get distal radius # Weber & Chao : as above Consistently reproduced # scaphoid in cadaveric wrists Frykman first showed that cadaver specimens were more likely to # scaphoid when wrist was HYPEREXTENDED AND RADIALLY DEVIATED If extensions angles less, more likely to get distal radius # Weber & Chao : as above Consistently reproduced # scaphoid in cadaveric wrists
- Baseline radiological investigation involves obtaining a good set of x-rays Up to 18 views have been described in literature but most authors concur that at least 4 to 5 views should be shot It is important to have a true PA and lateral view of the wrist The pronated view shows the half of the scaphoid best A look through the literature with regards to scaphoid view even then shows that there is no clear consensus with regards to how it should be performed, but many would agree that it is done with te wrist in ulnar deviation and 30 degree extension. Some would have the wrist in neutral with a beam centered over the capitate whilst others would shoot the film at a 20-25 degree cephalad direction It is reported that the fasle –ve rates of initial radiographs range between 2-25% and in clinically suspect cases, the appropriate management would be to cast and review in 2-3 weeks later with repeat radiographs and clinical assessment (Popularized by Watson Jones)
- The use of CT scans have been advocated by some authors as well, but its strengths lies in it’s ability to define the bony anatomy with clarity that supersedes radiographs and MRI In addition, CT scans are able to show the degree of bone loss/resorption in non-unions ncluding clarity demonstration of sclerosis of proximal pole fragments The scan is optimally performed along the longitudinal axis of the scaphoid with sagittal cuts about 1mm apart of 1-1.5mm thickness
- The MRI can detect occult fractures and reveal bone edema earlier than bonescans or radiographs and Fowler believes it to be more sensitive than the bonescan However it’s prime application lies in its use for assessing proximal pole vasculairty
- Combination of the Herbert and Russe classification gives a fair guide to treatment and Desai noted that using both Russe and Herbert classifications, there was a fair degree of inter and intra-observer reliability General principles are that Stable, undisplaced fractures heal quickly and well with low rates of non-union (virtually 100% union rate) Proximal pole fractures are notorious for delayed and non-union Trasverse waist fractures heal well But increasing obliquity and dorsal comminution indicates poorer mech stability and hence poorer healing
- Good article review by Barton on the late consequence of scaphoid fractures in JBJSB 2004 as well as Kozin who wrote the opening chpt Incidence, mechanism and natural history of scaphoid #s
- Barton reported in his review the work of previous authors including Amadio study of 46 patient of which 26 were found to have ISA of &gt;35 degrees Jiranek in JHSA 1992 compared 13 patients who had union following Russe grafts and 13 patients with malunion following Russe grafts Grip strength 90 to 76%, and wrist motion 90 to 78%
- so unlikely to require any form of reduction but merely protection Wrist position – in practice not so impt as if conserv rx in cast, generally undisplaced & stable # little effect on union rates (2) Type of cast- thumb involved? Elbow involved? Generally it is felt that there is no need for the cast to extend to the elbow: Verdan in1956 insisted that an above elbow cast was essential to eliminate pronation and supination and hence intercarpal motion Stewart reported 436 fractures SATS in USAMC with 95% union rates Exclsuion of thumb may also be safe with Clay and Dias reporting in their paired prospective cohort study in 1991 on 292 patients; with or without thumb immobilization, union rates were the same as was time to union Reliance on radiographs alone may also be unreliable. Dias has shown that intraobserver and interobserver reliability in evaluating union at 12 weeks is poor
- There is an increasing trend towards fixation of proximal pole fractures Surgical treatment of the acute scaphoid fracture may be done in a myriad fashions, including, open, closed, percutaneous as well as arthroscopic techniques The last mongram depicts an external fixator device applied for scaphoid fracture in 7 patients in a clinical trial of mixed distal waist and proximal fractures, external fixator device removed at 12 weeks. 100% union at 10 month follow up with good symptom score
- Below elbow cast for 28 days