Short cases in CVS: in paediatrics-final MBBS
•Download as DOCX, PDF•
12 likes•4,510 views

This is not a complete note or a guide. This was prepared by me based on the teachings of Dr.R.M.Mudiyanse just to aid the short cases.
![Effect on growth
Comment on current wt centile
Growth pattern: flattening, crossing centiles
FTT → ↑ BMR is due to symp overactivity
Difficulty in feeding/ frequent vomiting/ recurrent chest infection/ associated other anomalies
Reasons for tachypnea
Cong ht dx are associated with tachypnea
1. HF: rapid shallow breathing/ not much effort of breathing/ fine crepts/ cardiomegaly/ hepatomegaly/
m/
2. RTI: recession/ ↑ effort/ noises
3. Or both
Size & extent of the lesion
1. ANY complication→ means lesion is large→ needs Sx
2. Intensity of heart M does NOT correlate with size of the lesion. (loud M does not mean that lesion is
small or large)
3. Apical mid diastolic M [(functional M) in large VSD/ PDA] indicates pulm circulation is twice the
systemic circulation: blood is shunted to R/S(pulm vasculature)→ comes back to LA→ LV. Sx is
needed. So with VSD comment that no mid diastolic M in mitral area.
Comprehensive diagnosis
1. Complex cyanotic ht dx with growth failure probably has had a embolism in brain.
2. Large VSD or AV canal defect with pulm HTN & FTT in a child with trisomy 21, probably has LRTI also.
[If young mother is nearby, “young mothers have higher chance of having translocation than older
mothers, therefore I offer this mother karyotyping bcz of the usefulness of that information in the
process of counseling.” ]
Yapa Wijeratne M/07/189](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Short cases in CVS: in paediatrics-final MBBS
Similar to Short cases in CVS: in paediatrics-final MBBS (20)
More from Yapa
More from Yapa (20)
Recently uploaded
Recently uploaded (20)
Short cases in CVS: in paediatrics-final MBBS
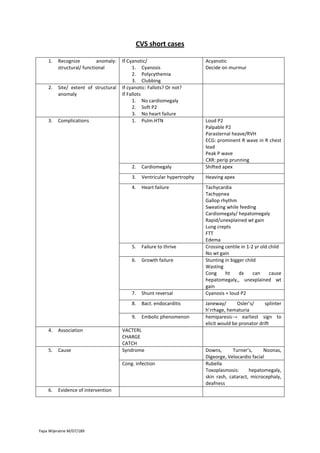
- 1. CVS short cases 1. Recognize anomaly: structural/ functional 2. Site/ extent of structural anomaly 3. Complications If Cyanotic/ 1. Cyanosis 2. Polycythemia 3. Clubbing If cyanotic: Fallots? Or not? If Fallots 1. No cardiomegaly 2. Soft P2 3. No heart failure 1. Pulm.HTN Acyanotic Decide on murmur 2. 3. Failure to thrive Growth failure 7. Shunt reversal Tachycardia Tachypnea Gallop rhythm Sweating while feeding Cardiomegaly/ hepatomegaly Rapid/unexplained wt gain Lung crepts FTT Edema Crossing centile in 1-2 yr old child No wt gain Stunting in bigger child Wasting Cong ht dx can cause hepatomegaly,, unexplained wt gain Cyanosis + loud P2 8. Bact. endocarditis 9. Cause Heart failure 6. 5. Heaving apex 5. Association Ventricular hypertrophy 4. 4. Cardiomegaly Loud P2 Palpable P2 Parasternal heave/RVH ECG: prominent R wave in R chest lead Peak P wave CXR: perip prunning Shifted apex Embolic phenomenon VACTERL CHARGE CATCH Syndrome Cong. infection 6. Evidence of intervention Yapa Wijeratne M/07/189 Janeway/ Osler’s/ splinter h’rrhage, hematuria hemiparesis→ earliest sign to elicit would be pronator drift Downs, Turner’s, Noonas, Digeorge, Velocardio facial Rubella Toxoplasmosis: hepatomegaly, skin rash, cataract, microcephaly, deafness
- 2. Effect on growth Comment on current wt centile Growth pattern: flattening, crossing centiles FTT → ↑ BMR is due to symp overactivity Difficulty in feeding/ frequent vomiting/ recurrent chest infection/ associated other anomalies Reasons for tachypnea Cong ht dx are associated with tachypnea 1. HF: rapid shallow breathing/ not much effort of breathing/ fine crepts/ cardiomegaly/ hepatomegaly/ m/ 2. RTI: recession/ ↑ effort/ noises 3. Or both Size & extent of the lesion 1. ANY complication→ means lesion is large→ needs Sx 2. Intensity of heart M does NOT correlate with size of the lesion. (loud M does not mean that lesion is small or large) 3. Apical mid diastolic M [(functional M) in large VSD/ PDA] indicates pulm circulation is twice the systemic circulation: blood is shunted to R/S(pulm vasculature)→ comes back to LA→ LV. Sx is needed. So with VSD comment that no mid diastolic M in mitral area. Comprehensive diagnosis 1. Complex cyanotic ht dx with growth failure probably has had a embolism in brain. 2. Large VSD or AV canal defect with pulm HTN & FTT in a child with trisomy 21, probably has LRTI also. [If young mother is nearby, “young mothers have higher chance of having translocation than older mothers, therefore I offer this mother karyotyping bcz of the usefulness of that information in the process of counseling.” ] Yapa Wijeratne M/07/189